© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
REMINISCENCE: ARTEFACTS FROM THE HKMMS
Halo-pelvic traction: a means of correcting severe spinal deformities
Louis CS Hsu, FHKAM (Orthopaedic Surgery)
Guest Author, Education and Research Committee, Hong Kong Museum of Medical Sciences Society
 Full
paper in PDF
Full
paper in PDF
The ‘Halo’, a metal ring secured with four screws
into the outer dipole of the skull, was popularised by
Perry and Nickel in the 1970s for prolonged cervical
traction in place of the old-fashioned, two-screw
skull tongs used in cervical fractures. With pins
inserted into the lower femur, they devised the halofemoral
traction for correction of spinal deformities.
This proved to be inefficient and the femoral pins got
infected very easily. The patient also had to remain in
bed during the traction.
With extension of the Sandy Bay Convalescent
Home to become the Duchess of Kent Children’s
Hospital in the late 1960s, Prof A Hodgson, Prof
A Yau, and Dr J O’Brien developed the pelvic
attachment of the halo-pelvic traction (HPT) device.
The pelvic ring is secured to the two halves of the
pelvis by two threaded pins that traverse the whole
length of the two halves of the pelvis. Extension bars
fitted to the halo and pelvic rings provide fixation
and traction when the bars are gradually elongated.
The apparatus provided very powerful corrective
forces (Fig 1a). It also allowed the patient to remain
ambulant during treatment (Fig 2).
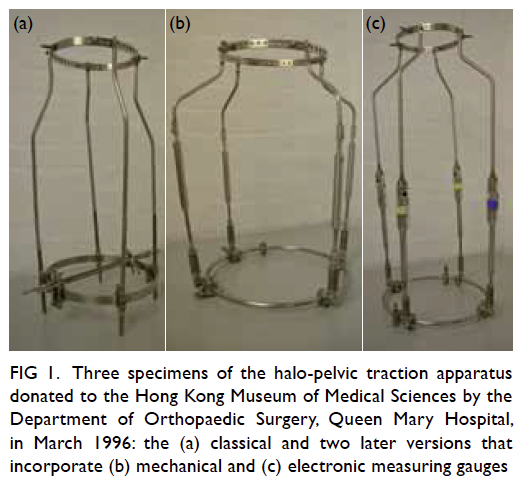
Figure 1. Three specimens of the halo-pelvic traction apparatus donated to the Hong Kong Museum of Medical Sciences by the Department of Orthopaedic Surgery, Queen Mary Hospital, in March 1996: the (a) classical and two later versions that incorporate (b) mechanical and (c) electronic measuring gauges

Figure 2. Photographs of patients in the Duchess of Kent Children’s Hospital with the apparatus in situ
In the later stages of the HPT improvement,
gauges attached to extension bars were used to
measure the forces generated through the spine
and helped the surgeons to monitor and regulate
the speed of distraction. Initially, the gauges were a mechanical compression spring attached to the
bottom of the bars (Fig 1b). Later, electrical cells
were used and attached to the middle of the bars
(Fig 1c).
Halo-pelvic traction was ideal for the treatment
of severe and rigid spinal deformities such as healed
tuberculous kyphosis. The strong fixation allowed
osteotomies of the rigid deformity to be staged and
distraction forces to be gradually applied between
stages of surgery without fear of instability or spinal
cord compression (Fig 3).
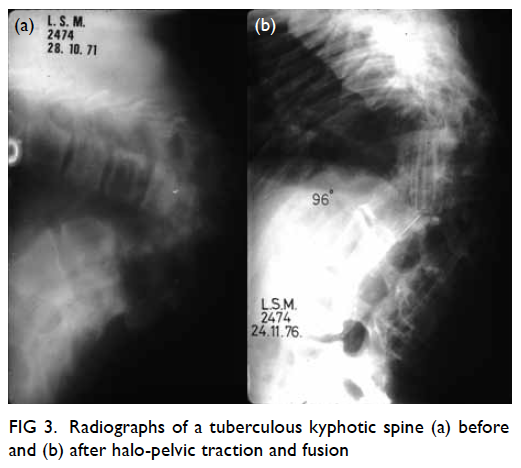
Figure 3. Radiographs of a tuberculous kyphotic spine (a) before and (b) after halo-pelvic traction and fusion
The apparatus can also be used for corrective
treatment of various types of severe scoliosis such
as that due to neurofibromatosis and poliomyelitis.
Again, the powerful distraction forces generated
can provide very dramatic correction of the rigid
deformities. Spinal fusions are performed after
correction of the deformities (Fig 4).
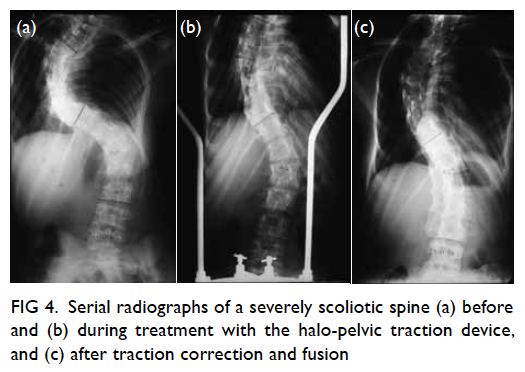
Figure 4. Serial radiographs of a severely scoliotic spine (a) before and (b) during treatment with the halo-pelvic traction device, and (c) after traction correction and fusion
Spinal tuberculosis and poliomyelitis epidemics
in Hong Kong in the 1950s and 60s left the region
with a significant number of patients with rigid spinal
deformities. Halo-pelvic traction came at the right
time as many patients could be appropriately treated
with this apparatus. Over 150 patients received HPT
treatment at the Duchess of Kent Children’s Hospital
during 1970 to 1982. All of them had severe spinal
deformities. They usually wore the apparatus for 3 to
6 months, and a few of them for up to a year.
However, the powerful distraction forces
along the spine, which houses the spinal cord, and
prolonged immobilisation resulted in some alarming
and unexpected complications.
During distraction, stretching the spine also stretches the nerves that run from the skull to the
trunk. The cranial nerves, especially the sixth,
tenth, eleventh and twelfth, and the brachial plexus,
especially the fifth and sixth nerve roots, can suffer
from traction injuries. In kyphotic patients, the spinal
cord may also be compressed by internal kyphus.
Detected early, these patients usually recover. Daily
neurological examination is an important routine in
managing the patients.
The cervical spine, being the most flexible part
of the spine, can be dramatically elongated by HPT.
The spinal cord may not keep pace. A small number
of patients with tuberculous kyphosis, despite a
gradual and slow distraction, suddenly developed
swinging temperatures and fluctuating rises in
blood pressure. These changes were attributed to
an early ‘coning’ of the medulla oblongata through
the foramen magnum, causing disturbances in the
temperature and blood pressure control centres.
These were quickly reverted by loosening the
distraction; the patients had no long-term effects
from these episodes.
An unexpected complication was discovered in
the odontoid process of the second cervical vertebra.
The blood supply to this process is essentially derived
from ligaments attached to this bone. With tension
in the ligaments from distraction, blood supply to the
odontoid process is jeopardised leading to avascular
necrosis. This was a rather common complication in
HPT. The necrosis itself recovered, but stiffness and
early degeneration of the cervical spine developed in
almost all of the patients.
Powerful traction to the flexible and fragile
cervical spine would cause minor damages to
the intervertebral ligaments and discs leading
to mild swelling, bleeding, and inflammatory
changes. Together with prolonged immobilisation,
spontaneous fusion had occurred in the cervical
spine in some patients.
With improvements in public health,
especially with infectious disease control and school
screening programmes for spinal deformities, severe
deformities requiring surgery are becoming rare. The
HPT device is now very rarely used, if at all, in Hong
Kong and in the rest of the world. Like many other
surgical instruments and equipment, it has become a
historical relic, though the service it provided to the
many deformed patients earns it a place in the Hong
Kong Museum of Medical Sciences.
References
1. O’Brien JP, Yau AC, Hodgson AR. Halo pelvic traction: a technic for severe spinal deformities. Clin Orthop Relat
Res 1973;93:179-90. CrossRef
2. Dove J, Hsu LC, Yau AC. The cervical spine after halo-pelvic traction. An analysis of the complications of 83
patients. J Bone Joint Surg Br 1980;62-B:158-61.
3. Yau AC, Hsu LC, O’Brien JP, Hodgson AR. Tuberculosis kyphosis: correction with spinal osteotomy, halo-pelvic
distraction, and anterior and posterior fusion. J Bone Joint Surg Am 1974;56:1419-34.