Exerting an impact on clinical practice—upholding quality, visibility, and timeliness of publications
DOI: 10.12809/hkmj175063
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
EDITORIAL
Exerting an impact on clinical practice—upholding
quality, visibility, and timeliness of publications
Martin CS Wong, MD, MPH
Editor-in-Chief, Hong Kong Medical Journal
 Full
paper in PDF
Full
paper in PDF
Since its inception in 1995, the Hong Kong Medical
Journal has evolved to have an official impact factor
in the Journal Citation Report, and it continues to be
a flourishing academic journal. Over the last 6 years,
the number of articles we received has increased by
52% to 440 in 2016, and the total number of non-local
articles submitted has risen drastically by 320%.
This is a true reflection of the journal’s increasing
popularity in the clinical and academic communities.
The acceptance rate has decreased from 50% to less
than 30%, reflecting the inevitably more rigorous
and stringent criteria applied in the evaluation of
all submissions. Our heartfelt gratitude goes to the
capable and visionary leadership of our past Editors-in-Chief, Dr CK Lee, Dr YL Yu, Dr Richard Kay, and
Prof Ignatius Yu who have undoubtedly laid a solid
foundation for our Journal. We are also appreciative
of the relentless efforts of our editorial members
and reviewers, both locally and internationally, who
have jointly made the journal to be one with growing
prestige and quality.
In previous inaugural and valedictory editorials
by our past Editors-in-Chief,1 2 3 4 5 the importance
of articles making an impact, whether on clinical
practice, public health policy or future research, has
been repeatedly emphasised. I believe this still holds
very true as it is an ultimate aspiration of all authors
who are determined to publish their original works.
One major question remains to address—how can we
make our published articles more influential? As the
new Editorial Board is appointed, we have in mind
three important criteria that we consider crucial:
quality, visibility, and timeliness of publication.
We are most interested in articles that are of
high methodological quality. To further make this a
top priority in the coming years, the editorial team
will place an increasing weight on the quality of the
research methodology when they make editorial
decisions. The peer reviewer report has been
modified to ensure this is an overriding criterion for
article acceptance. In particular, we have solicited
more support from senior members of the Editorial
Board, together with the our epidemiology and
biostatistics advisors, to rigorously review and
clarify the methodological details of all provisionally
accepted original articles well before they are
formally published. We hope that this process will
help strengthen the validity and presentation of
the information we publish. Apart from original
research papers, we solicit high-quality reviews
as well as medical practice papers that describe
recent technological advances or summarise
current guidelines for addressing common medical
problems. We hope these papers will help readers in
their daily practice.
Another important aspect of our future work
is to enhance the visibility of our journal articles.
Without effective dissemination, no high-quality
articles can realise their actual impact. The initiative
began in 2015 when a responsive, user-friendly, web
technology was built to enhance browsing of the
journal via desktops, smartphones, and tablets. The
“online first” feature of the publication since 2013
is yet another attempt to make our articles easily
accessible. Our senior editors will also offer advice
for authors to make their articles more “search engine
optimised”6 by suggesting potential modifications
to the keywords of all original contributions as
displayed in MEDLINE versions. We do of course
recommend that our authors present their findings
at academic conferences, share them with their
colleagues and appropriate social media, and expand
their professional network.
Timely publication is a crucial aspect, and
indeed responsibility, of every academic journal to
ensure efficient dissemination of research findings.
In the coming years, our editorial members will
be working towards the target of making the first
editorial decision of whether to send a paper for
external peer review within an average of 15 working
days for all original articles. Whilst this requires very
diligent and committed work from all Editorial Board
members, we believe this initiative is worthwhile.
Authors as well as readers will welcome the reduced
time between acceptance of a manuscript and its
appearance in our Journal via expeditious review.
We strongly believe that HKMJ will continue
to be an internationally world-class academic journal
that publishes articles of “high quality reflecting the
current practice in the science and art of medicine
and public health”.5 We are also confident that
the Journal will continue the proud history over
32 years of the Journal of the Hong Kong Medical
Association and its predecessors in “providing a
useful source of medical information on advances
in medical research and clinical practice.”5 To this
end, we must emphasise that the continuing support
of our international advisors, board members,
editorial staff, reviewers, authors, and all Academy
Fellows is essential. To quote our Immediate Past
Editor-in-Chief Prof Ignatius Yu, we sincerely “call
on your continued love and support”2 to make the
Journal a great success. We are always attentive and
appreciative of your invaluable comments, and of
course your submissions.
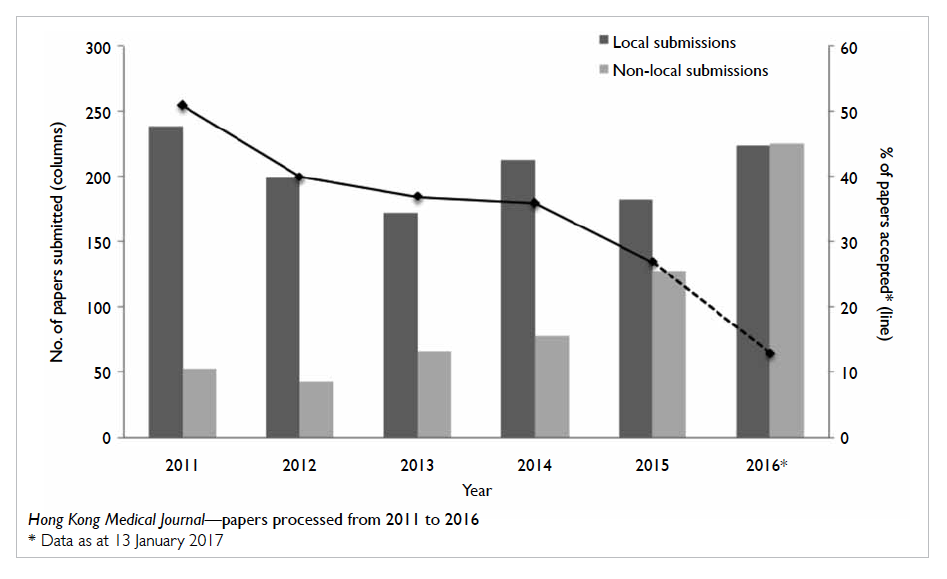
Hong Kong Medical Journal—papers processed from 2011 to 2016
References
1. Yu IT. Helping the Hong Kong Medical Journal and Hong
Kong to advance their impact on medical practice. Hong
Kong Med J 2016;22:524-5. Crossref
2. Yu IT. Calling on your continued love and support. Hong
Kong Med J 2011;17:4.
3. Yu YL. Building upon a firm foundation. Hong Kong Med J
2001;7:4.
4. Kay R. Valedictory remarks. Hong Kong Med J 2010;16:420.
5. Lee JC, Yu YL. Inaugural editorial. Hong Kong Med J
1995;1:4.
6. Burger M. How to improve the impact of your paper.
Available from: https://www.elsevier.com/authors-update/story/publishing-tips/how-to-improve-the-impact-of-your-paper. Accessed 29 Dec 2016.