Hong
Kong Med J 2019 Oct;25(5):407.e1–2
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Sudden cardiac arrest with pericardial contrast during
computed tomography aortogram in a type A aortic dissection
patient
WM Yu, MB, ChB, FRCR1; WL Wong, MB, ChB, FRCR1; FH Ng, MB ChB,
FRCR2
1 Department of Radiology, United
Christian Hospital, Kwun Tong, Hong Kong
2 Department of Radiology, Caritas
Medical Centre, Shamshuipo, Hong Kong
Corresponding author: Dr WM Yu (wenmingyu@hotmail.com)
 Full
paper in PDF
Full
paper in PDF
A 69-year-old man with long-standing hypertension
and history of pulmonary embolism on warfarin presented to Accident and
Emergency Department with sudden upper back pain and transient loss of
consciousness. On admission, the patient was in haemodynamic shock with
blood pressure 83/57 mm Hg and pulse 42 beats per minute. Cardiovascular
examination revealed radial-radial and radial-femoral delay.
Electrocardiogram showed complete heart block and chest radiograph
demonstrated a widened mediastinum. An immediate bedside echocardiogram
found an intimal flap in the aortic root with evidence of aortic
regurgitation and a thin rim of pericardial effusion.
Fluid resuscitation and inotropic support was given
and urgent computed tomography (CT) aortogram was arranged to further
delineate the extent of involvement of aortic dissection. However, the
patient developed sudden cardiac arrest immediately after being given 80
mL intravenous Omnipaq at a rate of 3 mL/s via injector during CT
aortogram. A review of CT images showed Stanford type A aortic dissection
with an intimal flap extending into the pericardial sac (Fig
1). No obvious pericardial effusion was visible on the pre-contrast
CT images (Fig 2a). However, significant contrast was seen in
the pericardial sac on post-contrast CT images (Fig 2b), indicating a sudden rupture with
haemopericardium had occurred during the CT scan. Despite prompt bedside
pericardiocentesis and cardiopulmonary resuscitation, the patient died.
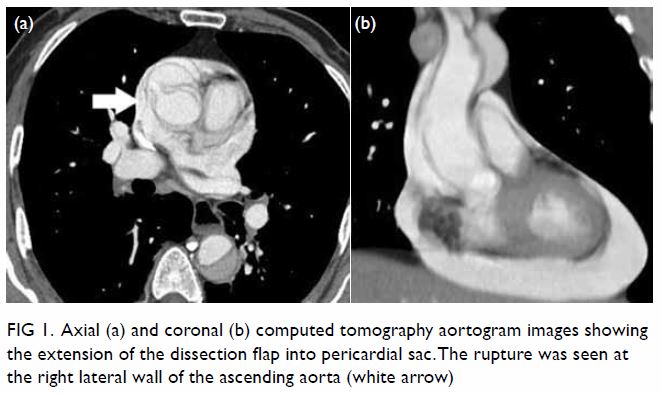
Figure 1. Axial (a) and coronal (b) computed tomography aortogram images showing the extension of the dissection flap into pericardial sac. The rupture was seen at the right lateral wall of the ascending aorta (white arrow)
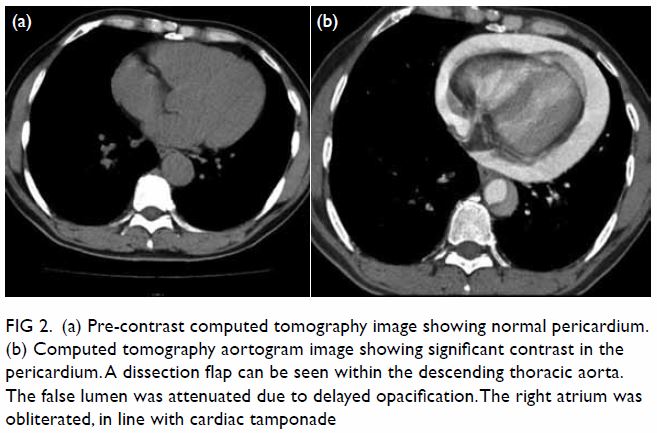
Figure 2. (a) Pre-contrast computed tomography image showing normal pericardium. (b) Computed tomography aortogram image showing significant contrast in the pericardium. A dissection flap can be seen within the descending thoracic aorta. The false lumen was attenuated due to delayed opacification. The right atrium was obliterated, in line with cardiac tamponade
Aortic dissection is the most common acute
emergency condition of the aorta. The mortality rate is high, and rupture
is the cause of death in approximately one-third of affected patients.1 The pathology is due to a tear in the intimal layer
allowing blood to propagate into the media and create a false lumen. In
the ascending thoracic aorta, the primary tear is most often within 3 cm
of the aortic cusps.2 The false
lumen of aorta may rupture due to loss of elastic recoil and increased
wall stress with dilatation. Often, the rupture site is close to the
initial intimal-medial tear over the right lateral wall where it receives
the ejected blood from the left ventricle.2
This ends up into the pericardial sac causing haemopericardium and
subsequent fatal cardiac tamponade.2
Computed tomography aortogram is the first-line
modality in the diagnosis of aortic dissection, delineation of its extent
of involvement and end-organ ischaemia. In our case, rupture of the aorta
into the pericardial sac was evidenced by significant contrast-enhanced
haemopericardium on CT aortogram images which was absent in pre-contrast
CT images. This could be related to the rapid injection of a large volume
bolus of intravenous contrast by power-injector, resulting in a sudden
elevation of left ventricular pressure, supported by previous study in
human subjects demonstrating a significant increase in blood pressure
after bolus injection of low osmolarity, non-ionic contrast agent.3
The treatment of type A aortic dissection with
rupture is immediate surgical repair.4
5 Although it was previously
considered controversial to perform pericardiocentesis as there is a risk
of worsening the leak, recent evidence suggests that controlled
pericardiocentesis may reduce haemodynamic instability in critical cardiac
tamponade to allow sufficient time for urgent operative repair.5
Author contributions
WM Yu and FH Ng are responsible for the concept of
study, acquisition and analysis of data, and drafting of the article. All
authors are responsible for critical revision for important intellectual
content. All authors had full access to the data, contributed to the
study, approved the final version for publication, and take responsibility
for its accuracy and integrity.
Conflicts of interest
All authors have disclosed no conflicts of
interest.
Funding/support
This research received no specific grant from any
funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
The present study was reviewed and approved by the
Kowloon Central Cluster/Kowloon East Cluster Research Ethics Committee
(KCC/KEC-2019-0179). Because the concerned patient was deceased, the
requirement for consent was waived by the ethics board.
References
1. Mehta RH, Suzuki T, Hagan PG, et al.
Predicting death in patients with acute type a aortic dissection.
Circulation 2002;105:200-6. Crossref
2. Patel YD. Rupture of an aortic
dissection into the pericardium. Cardiovascular Intervent Radiol
1986;9:222-4. Crossref
3. John AM, Yadar S. Evaluation of blood
pressure variations during the administration of intravascular contrast
media in CECT Abdomen. Asian J Pharm Clin Res 2018;11:309-11. Crossref
4. Adler Y, Charron P, Imazio M, et al.
2015 ESC Guidelines for the diagnosis and management of pericardial
diseases: The Task Force for the Diagnosis and Management of Pericardial
Diseases of the European Society of Cardiology (ESC). Endorsed by: The
European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J
2015;36:2921-64. Crossref
5. Hayashi T, Tsukube T, Yamashita T, et
al. Impact of controlled pericardial drainage on critical cardiac
tamponade with acute type A aortic dissection. Circulation. 2012;126(11
Suppl 1):S97-S101. Crossref