Hong Kong Med J 2024 Feb;30(1):33–43 | Epub 19 Feb 2024
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Dietary habits and physical activity during the third wave of the COVID-19 pandemic: associated factors, composite outcomes in a cross-sectional telephone survey of a Chinese population, and trend analysis
Winnie YY Lin, MS, RDN1,2; Martin CS Wong, MD, MPH3; Junjie Huang, MD, MSc3; Yijun Bai, MPH3; Siew C Ng, MB, BS, PhD1,2,4; Francis KL Chan, DSc, MD2,5
1 Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Hong Kong SAR, China
2 Microbiota Innovation Center, Hong Kong SAR, China
3 The Jockey Club School of Public Health and Primary Care, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, China
4 State Key Laboratory of Digestive Disease and Institute of Digestive Disease, The Chinese University of Hong Kong, Hong Kong SAR, China
5 Centre for Gut Microbiota Research, The Chinese University of Hong Kong, Hong Kong SAR, China
Corresponding author: Ms Winnie YY Lin (winnielin@cuhk.edu.hk)
 Full paper in PDF
Full paper in PDF
Abstract
Introduction: The coronavirus disease 2019
(COVID-19) pandemic created many challenges for
Hong Kong residents attempting to maintain healthy
lifestyle habits. This study aimed to measure the
prevalences of unhealthy dietary habits and physical
inactivity levels in Hong Kong Chinese, identify
associated factors, and conduct a time trend analysis
during the third wave of the COVID-19 pandemic.
Methods: A cross-sectional telephone survey
was conducted in Hong Kong by simple random
sampling. The survey comprised socio-demographic
characteristics, clinical information, the Hong
Kong Diet Score (HKDS), smoking and alcohol
consumption, and a Chinese version of the
International Physical Activity Questionnaire
Short Form. The composite outcome was low
HKDS, physical inactivity, smoking, and alcohol
consumption. We used 14 Health Behaviour Survey
reports from 2003 to 2019 to establish a trend analysis
regarding fruit and vegetable consumption, physical
activity level, smoking, and alcohol consumption.
Results: We performed 1500 complete telephone
surveys with a response rate of 58.8%. Most
participants were older adults (≥65 years, 66.7%),
women (65.6%), and married (77.9%). The HKDS was
significantly lower in men, single individuals, low-income
participants, alcohol drinkers, and patients with diabetes mellitus or renal disease. Participants
who were single, undergoing long-term management
of medical diseases, or had diabetes or renal diseases
exhibited greater likelihood of physical inactivity.
Conclusion: Prevalences of unhealthy lifestyle
habits were high among men, single individuals, and
chronic disease patients during the third wave of the
COVID-19 pandemic in Hong Kong. The adoption
of physical activity habits tended to decrease in the
past two decades.
New knowledge added by this study
- This population-based survey indicated that a larger proportion of Hong Kong residents, compared with pre-pandemic years, had a non-healthy lifestyle during the third wave of the coronavirus disease 2019 pandemic.
- Majority of participants had a low Hong Kond Diet Score, suggesting minimal adherence to the traditional Chinese eating pattern; these participants were mainly younger individuals and men.
- There is an urgent need to formulate and implement effective public health strategies at both individual and organisational levels. The encouragement of healthy lifestyles through evidence-based health promotion programmes is essential, which could be conveyed to communities through organised and concerted efforts by the government and relevant stakeholders.
- Future studies should evaluate the effectiveness of various interventions and approaches to achieve these important goals.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic
has affected >770 million people worldwide, causing >7 million deaths as of 31 December 2023.1 The
period between July and September 2020 constituted
the third wave of the pandemic in Hong Kong, resulted in >1.2 million reported cases between 23
January 2020 and 29 January 2023.2 The containment
strategies implemented during the third wave
included mandatory mask wear in public places, even
when exercising in public outdoor areas; suspensions
of public leisure facilities and private gyms; and the
initiation of work-from-home arrangements.3 These
strategies led to reductions in physical activity and
daily movement, with the goal of viral containment.
Furthermore, compulsory social distancing and
suspension of dine-in services were included among
the policies that could affect various dietary and
lifestyle habits, although these methods were less
stringent than approaches in cities under lockdown.
Overall, the unprecedented public health crisis
created many challenges for Hong Kong residents
attempting to maintain healthy lifestyle habits.
Nevertheless, few studies have examined dietary
and physical activity habits in the general population
during the COVID-19 pandemic.4 5 6
Considering that individuals with chronic
diseases are more likely to develop severe cases
of COVID-19, this study aimed to measure the
prevalences of unhealthy dietary habits and physical
inactivity levels in an adult Chinese population,
to identify factors associated with their adoption
of these dietary and physical activity habits, and
to perform a time trend analysis comparing the
proportions of the population that adopted healthy
dietary habits, physical activity levels, and avoidance of smoking and alcohol consumption during the
third wave of the COVID-19 pandemic.
Methods
Sampling
We utilised a methodology similar to a previous
population-based, random telephone survey
conducted in Hong Kong.7 Two-stage sampling was
performed, in which participants were recruited by
trained interviewers through a telephone interview
system based on telephone calls to landlines identified
by random digit dialling. The sample population
was randomly selected by the Centre for Health
Behaviours Research at The Chinese University of
Hong Kong. Calls were made during typical office
hours, 9 am to 5 pm, Monday through Saturday
between 7 and 31 October 2020. Three attempts
were made if the call initially was not answered.
Territory-wide, any Chinese adults aged ≥18 years
who could communicate in Chinese via telephone
were eligible to participate. Assuming an outcome
variable rate of 35%, at least 1456 participants were
required to achieve a precision level of 2.5% from the
following formula:

where ‘p’ stands for proportion and ‘N’ stands for sample size.
The interviews were performed using a
fieldwork manual highlighting standard operating
procedures by a team of trained interviewers and
supervised by an experienced project coordinator
throughout the study. The characteristics of survey participants are shown in Table 1.
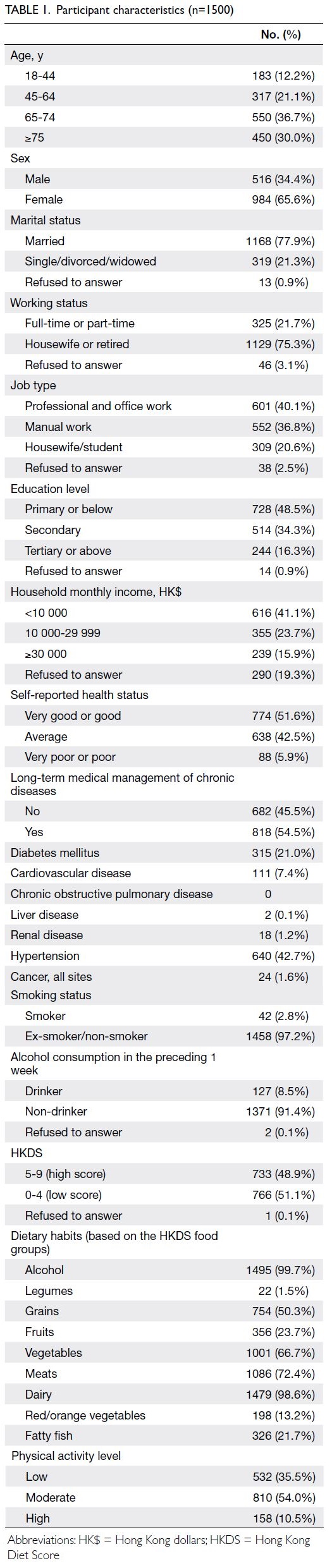
Table 1. Participant characteristics (n=1500)
Survey instrument
The survey consisted of five sections: (1) socio-demographic
details (age, sex, marital status,
education level, job status, household income, and
receipt of comprehensive social security assistance);
(2) clinical information (eg, presence of chronic
diseases); (3) smoking (current daily amount/ex-/non-smoker) and alcohol consumption habits
(daily amount in the preceding 7 days); (4) dietary
screening via the Hong Kong Diet Score (HKDS),
using a validated scale that contained nine items
assessing the participant’s daily consumption of
nine food groups in the preceding 7 days; and (5)
level of physical activity in the preceding 7 days,
as determined by a Chinese version of the 7-item
International Physical Activity Questionnaire Short
Form (IPAQ-C).
Scoring of the Hong Kong Diet Score, International Physical Activity Questionnaire, and unhealthy lifestyle score
The traditional Mediterranean diet is well-defined and has been positively associated with favourable
health outcomes.8 9 10 The Mediterranean diet score is used to measure compliance with a traditional
Mediterranean diet. This scoring system has been
widely utilised in studies that measure Mediterranean
diet adherence or adaptation as an indicator of
healthy dietary choices. In this study, we developed
the HKDS, a dietary screener that contained nine
items assessing dietary intake of nine food groups
(alcohol, legumes, grains, fruits, vegetables, meats,
dairy, red/orange vegetables, and fatty fish) in the
preceding 7 days. The screener incorporated key
traditional Greek diet characteristics, known as the
Mediterranean diet score of de Groot et al,8 which
were also used in a study of Hong Kong Chinese by
Woo et al (Table 2).11 The original 8-item survey was
modified by removing the ratio of monounsaturated
fatty acids to saturated fatty acids and replacing
ethanol with alcohol. Dietary fatty acids and ethanol
are widely distributed among various food groups;
they are typically assessed through weighted foods,
which are unlikely to be accurately determined using
a single question in a telephone interview. Two
additional items were included regarding carotenoid-rich
and omega-3–rich food intake based on the
Hong Kong Centre for Food Safety Recommended
Nutrient Intake for vitamin A12 and the World Health
Organization recommendation for omega-3. Both
nutrients are inversely associated with incidence of
non-communicable diseases (NCDs). For each item,
consumption at or above the recommended amount
was scored as 1 point and 0 points otherwise;
however, for ethanol, consumption below the
specified amount was scored as 1 point and 0 points
otherwise. Each participant received a total score
of 0 to 9; a score of ≥5 was considered high. A pilot
survey was conducted with a convenience sample
of 23 participants. Intraclass correlation coefficient
estimates and 95% confidence intervals (CIs) were
determined using a two-way mixed-effects model to
assess internal consistency regarding the number of
serves (ie, serving sizes of the food group consumed)
reported. The intraclass correlation coefficient
was 0.87, indicating good reliability. Cohen’s κ was
calculated to evaluate agreement between test and
retest scores. Agreement between the two tests was
fair (κ=0.24, 95% CI=-0.15 to 0.63; P=0.239).
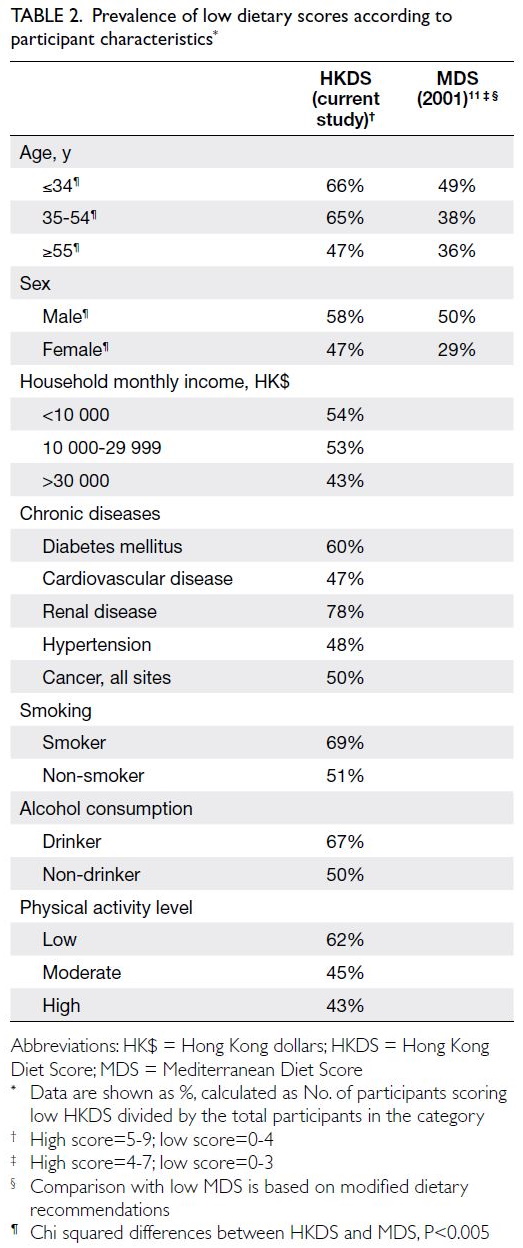
Table 2. Prevalence of low dietary scores according to participant characteristics
The IPAQ-C score was regarded as a
categorical variable indicating exercise level based
on the frequency and intensity of physical activity:
(1) low (total activity <600 metabolic equivalent of
task [MET]–minutes/week), (2) moderate (total
activity ≥600 MET-minutes/week), or (3) high (total
activity >3000 MET-minutes/week).
Finally, an unhealthy lifestyle score (0 to 4) was
assigned to each participant based on a composite
outcome involving low HKDS, physical inactivity,
current smoking habit, and alcohol consumption;
each unhealthy habit contributed 1 point to the
score.
Data analysis
We used SPSS software (Windows version 26.0; IBM
Corp, Armonk [NY], United States) for data analysis.
Descriptive analyses were performed regarding the
participants’ socio-demographic details, clinical
information (eg, presence of chronic diseases), and
the HKDS. The primary outcome variables included:
(1) unhealthy dietary habits (low HKDS score); (2)
suboptimal physical activity (low IPAQ-C score,
indicating low exercise level); and (3) unhealthy
lifestyle score (≥2). Univariable logistic regression
was performed to examine associations between
socio-demographic variables and each of the first two
outcome variables. Multivariable logistic regression
was modelled by controlling for covariates with
P values <0.20 in univariable regression analysis,
a cut-off level commonly used in public health
research. For example, Torenfält and Dimberg13
utilised this approach when evaluating stroke and
death in middle-aged Swedish men. The approach
was also used in a French study14 concerning
medical features of patients with COVID-19 and
influenza. Additionally, linear regression analysis
was conducted in the present study to examine
associations between socio-demographic variables
and the unhealthy lifestyle score. Time trends for
various food intake, physical inactivity, current
smoking, and alcohol consumption statuses were
evaluated; the prevalences of these lifestyle habits
were compared with population-wide figures from
governmental reports over the past two decades
using the Chi squared test for heterogeneity. P values
<0.05 were considered statistically significant.
Data sources for time trend comparisons
The Centre for Health Protection has been
conducting health surveys periodically since 2003
to collect information about health and lifestyle-related
behaviours, as well as practices related to
the prevention of NCDs among residents aged ≥15
years.15 The resulting reports have presented key
findings concerning physical activity, dietary habits,
alcohol consumption, and smoking habits, as well
as other self-care practices. We gathered relevant
findings from 14 governmental reports covering the
period from 2003-2004 to 2018-2019 (calendar years
with the most updated figures)15 to perform trend
analysis of fruit and vegetable consumption, physical
activity level, smoking, and alcohol consumption
status among Hong Kong residents. These results
were compared with the findings of the present
study; adjustments were solely performed for sex
because the age distribution was limited in all but
the most recent reports.
Results
In total, 2551 individuals were contacted for a telephone interview and 1500 participated; the response rate was 58.8%.
Most interviewed individuals were older adults (≥65
years, 66.7%), women (65.6%), and married (77.9%). Of
the participants, 40.1% were engaged in professional
and office work; only 16.3% had attained a tertiary
education or higher. About 16% of participants
reported a household income ≥HK$30 000, whereas
41.1% reported a household income <HK$10 000.
Health status was predominately self-reported as
average (42.5%) or above average (51.6%). More than
half of the participants (54.5%) were undergoing
long-term medical management or were taking
medications for chronic diseases; the most common
chronic conditions were diabetes mellitus (21.0%)
and hypertension (42.7%) [Table 1].
Prevalence of low dietary score among Hong
Kong Chinese
Dietary habits, as measured by the HKDS (score range, 2-9), were classified as high scoring (5-9) or
low scoring (0-4). Approximately 51% of participants
had a low score (Table 1), suggesting minimal
adherence to the traditional Chinese eating pattern;
these participants were mainly younger individuals
(aged ≤34 years, 66%) and men (58%) [Table 2].
Greater proportions of participants with lower
income, current smokers, and current drinkers
had low scores according to the HKDS (54%, 69%,
and 67%, respectively) [Table 2]. Participants with chronic diseases had various HKDS results; <50% of
patients with renal diseases and diabetes had a high
score, and this result indicated that they had a poor
dietary habits.
Dietary habits and physical activity
A greater risk of practising unhealthy dietary habits (low HKDS) was associated with male sex
(adjusted odds ratio [aOR]=1.31, 95% CI=1.03-1.67),
non-married status (ie, single/divorced/widowed)
[aOR=1.56, 95% CI=1.20-2.03], a diagnosis of
diabetes (aOR=1.53, 95% CI=1.15-2.03), and alcohol
consumption (aOR=1.76, 95% CI=1.17-2.64) [Table 3].
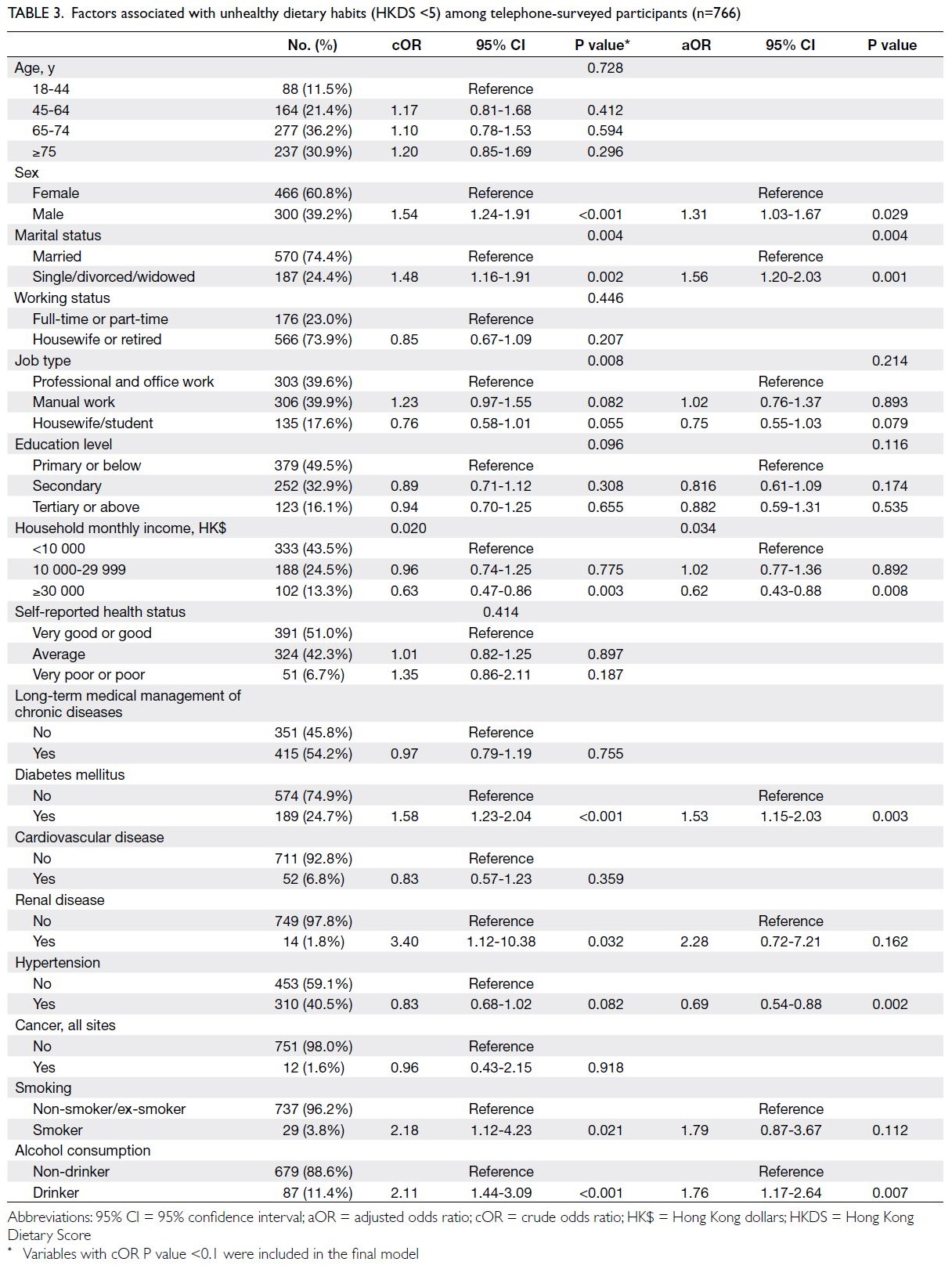
Table 3. Factors associated with unhealthy dietary habits (HKDS <5) among telephone-surveyed participants (n=766)
Among all participants, 35.5%, 54.0% and
10.5% had low, moderate, and high levels of physical
activity, respectively (Table 1). Participants who
were non-married (aOR=1.66, 95% CI=1.23-2.22),
undergoing long-term management of medical
diseases (aOR=1.65, 95% CI=1.08-2.54), had diabetes
(aOR=1.39, 95% CI=1.02 to 1.89), and had renal
diseases (aOR=9.32, 95% CI=2.06-42.25) exhibited
greater likelihood of physical inactivity (Table 4).
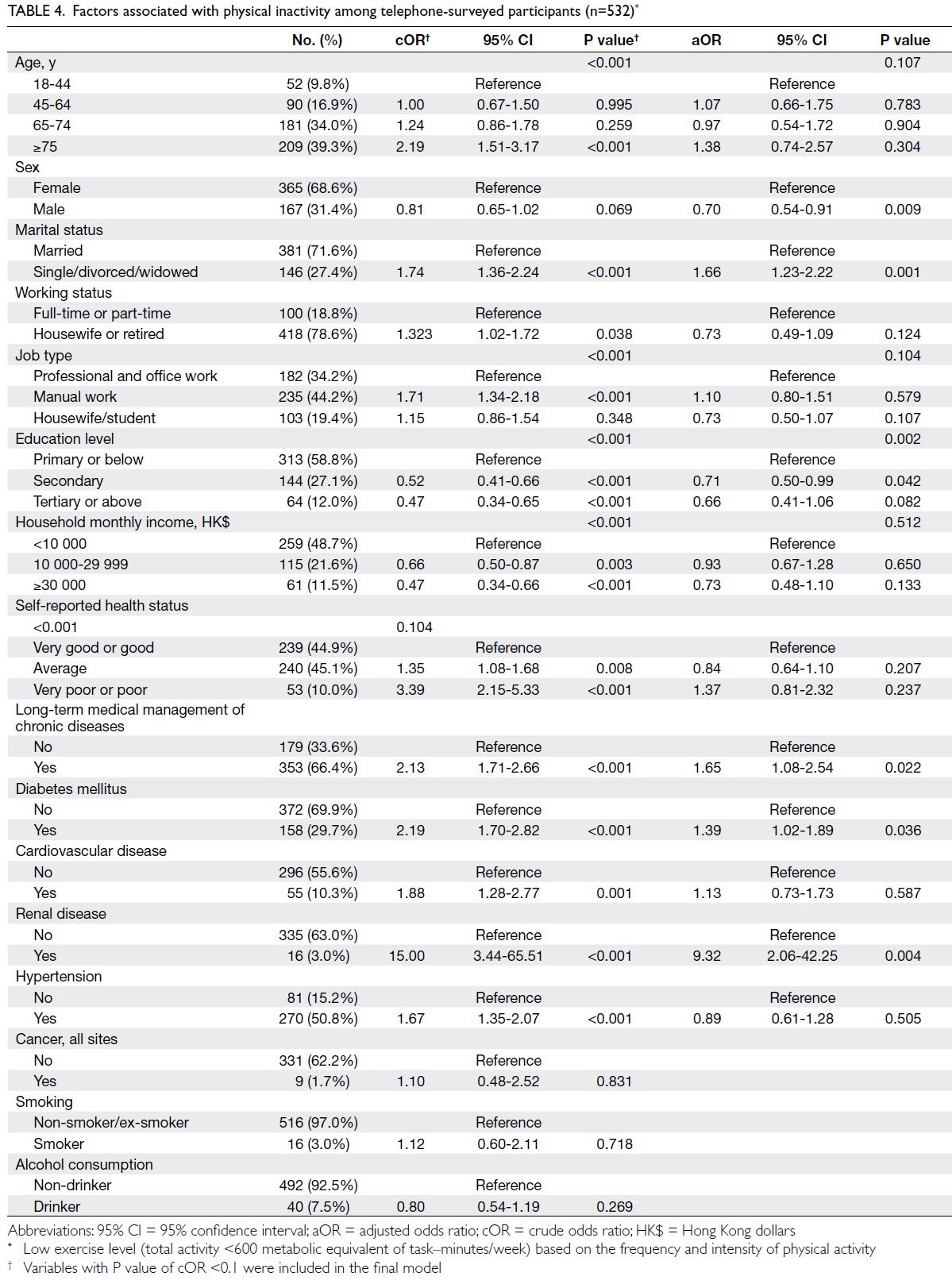
Table 4. Factors associated with physical inactivity among telephone-surveyed participants (n=532)
Other lifestyle habits: smoking and alcohol
Few participants were current daily smokers (2.8%) and alcohol drinkers (8.5%) [Table 1].
Factors associated with higher risk of an unhealthy lifestyle score
Factors associated with an unhealthy lifestyle score
are presented in Table 5. Male sex (beta coefficient
[β]=0.25, 95% CI=0.16-0.34), non-married status
(β=0.19, 95% CI=0.08-0.29), manual work (β=0.17,
95% CI=0.07-0.27), self-reported poor or very poor
health status (β=0.26, 95% CI=0.07-0.45), a diagnosis
of diabetes (β=0.31, 95% CI=0.20-0.41), and a
diagnosis of renal disease (β=0.92, 95% CI=0.53-1.31)
increased the likelihood of poor lifestyle habits.
Housewife or retired status (β=-0.15, 95% CI=-0.25 to
-0.04) and a higher household income (≥HK$30 000;
β=-0.20, 95% CI=-0.33 to -0.08) decreased the
likelihood of poor lifestyle habits.
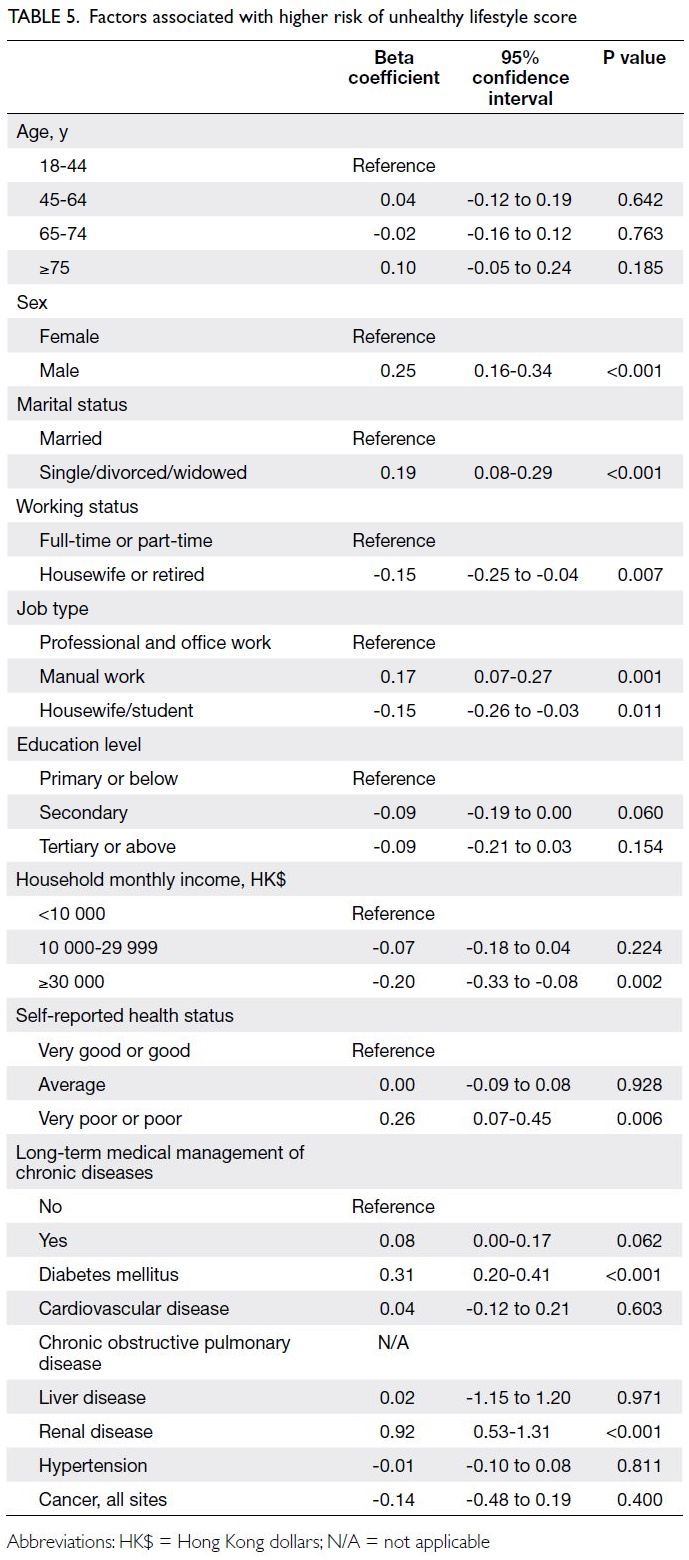
Table 5. Factors associated with higher risk of unhealthy lifestyle score
Time trend analysis of fruit and vegetable consumption, physical activity, smoking, and alcohol consumption
The Health Behaviour Survey, with a response rate
of 70.8% in the 2018/2019 report, is a population-based
fieldwork study conducted by the Centre for
Health Protection of the Department of Health.16
In that survey, female participants comprised 52.7%
of the sample, compared with 65.6% in the present
telephone survey. The age-group with the largest
proportion of participants in the Survey was 65 to 74
years (36.7% vs 11.0%), which might have influenced
the sex ratio.
Time trend analysis showed that the proportion
of surveyed Hong Kong residents eating five daily
servings of fruits and vegetables declined for both
sexes in general (Fig a). Similarly, a significantly
smaller proportion of participants reported walking
>10 minutes for ≥5 days per week, and this proportion
has continued to decline since 2016 (Fig b). There was
a gradual decrease in the number of participants with
a moderate or high level of physical activity. Despite
a notable peak in 2019, there was a decline in 2020
with <60% of participants reportedly engaging in
these physical activities. Finally, significantly smaller
proportion of the study participants reported not
currently smoking or consuming alcohol, compared
with the proportions in previous population-based
surveys (2010-2019) [Fig c and d].
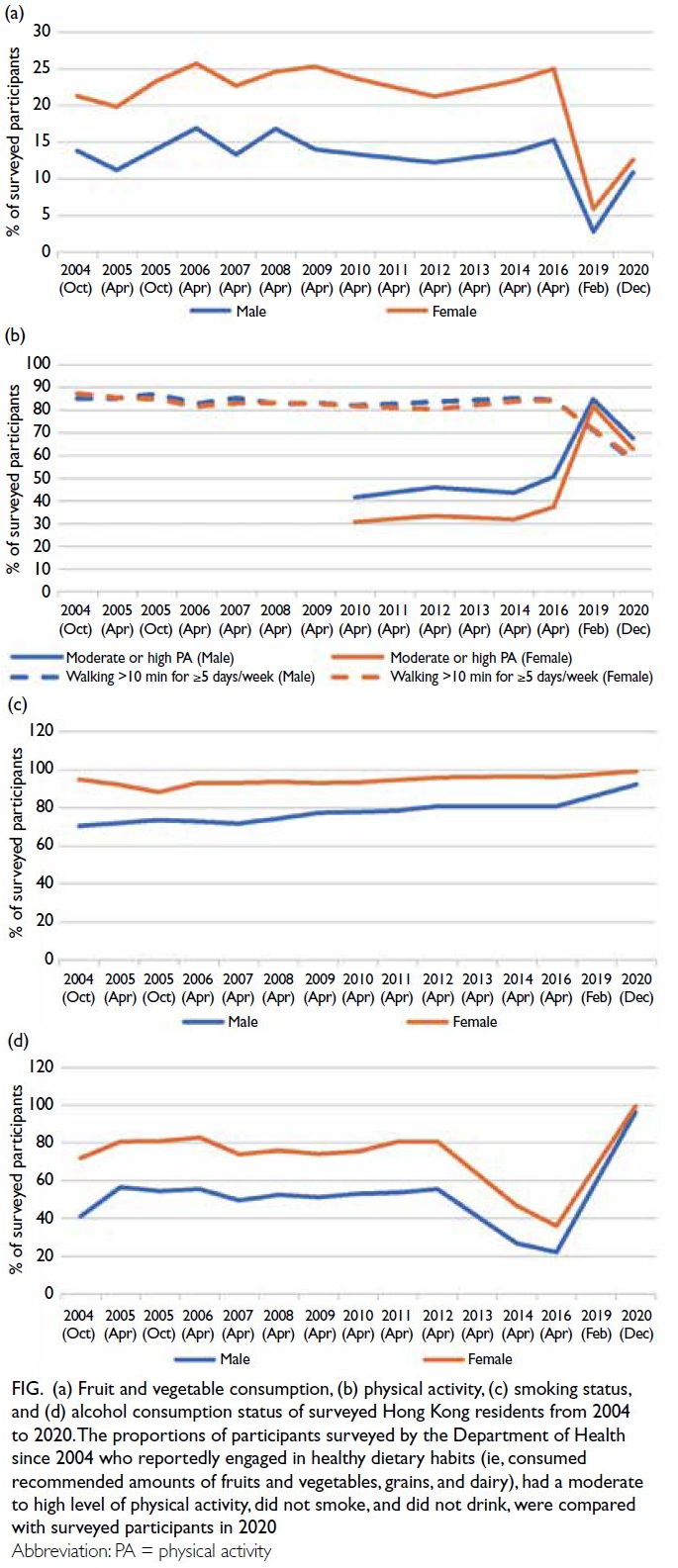
Figure. (a) Fruit and vegetable consumption, (b) physical activity, (c) smoking status, and (d) alcohol consumption status of surveyed Hong Kong residents from 2004 to 2020. The proportions of participants surveyed by the Department of Health since 2004 who reportedly engaged in healthy dietary habits (ie, consumed recommended amounts of fruits and vegetables, grains, and dairy), had a moderate to high level of physical activity, did not smoke, and did not drink, were compared with surveyed participants in 2020
Discussion
In this population-based study of 1500 Hong Kong
residents during the third wave of the COVID-19
pandemic, we found that the proportion of people
with healthy food intake (ie, daily consumption of
five servings of fruits and vegetables) has decreased
since 2003; although a slight increased was observed
in 2020, it was still below the overall average.
Additionally, we found that the prevalence of low
physical activity has gradually increased. In contrast,
the rates of smoking and alcohol consumption
were below the rates observed in pre-pandemic
population-based surveys. Men and women in
various age-groups had dietary habits less adherent
to the traditional Chinese eating pattern, as measured
by the HKDS, than 20 years prior. Adherence to the
traditional eating pattern was significantly lower
among male participants, single individuals, low-income
participants, alcohol drinkers, individuals
with low physical activity, and patients with diabetes
mellitus or renal disease. We also found that men,
individuals with non-married status, manual
workers, individuals with self-perceived poor or
very poor health status, and patients with diabetes
and renal disease had a greater likelihood of poor
lifestyle habits.
Worldwide, insufficient intake of fruits and
vegetables and inadequate physical activity have
been attributed to 34% and ≥20% of NCDs,
respectively.17 18 The incidence of chronic diseases
(eg, cancers, diabetes, and cardiovascular disease)
in Hong Kong has increased by 60% in the past two
decades.19 Although processed food intake was not
assessed in this study, the HKDS results indicated
very low intakes of legumes and red/orange
vegetables among Hong Kong residents; a previous
study showed that fruit intake in Hong Kong is
among the lowest levels worldwide.20 The report of
Health Behaviour Survey 2018/2019 revealed that 95.6% of surveyed participants had inadequate daily
fruit and vegetable intake, based on World Health
Organization recommendations.16 The present study
showed further reduction, such that the proportion of
Hong Kong residents consuming the recommended
(≥5) daily servings of fruits and vegetables declined
by 3.9% in the past two decades. Additionally, 10% of
the population reported consuming more than one
daily serving of processed meat, and the frequency
of processed meat consumption increased by 3.1%.16
Another known risk factor for NCDs, overweight
or obesity, affected approximately half of the Hong
Kong population aged 15 to 84 years in 2015; this
value was slightly (2%) below the global average.21
Disruptions to usual routines can lead to new
dietary behaviours. For example, dine-in restrictions
at restaurants and bars during the pandemic led to
greater use of food delivery services, and take-away
food is often less healthy.22 However, we observed
increased fruit and vegetable consumption after
the third wave of the COVID-19 outbreak. This
finding is supported by the work of Wang et al,23
which showed that fruit and vegetable consumption
increased. Collectively, the disease prevention and
control policies that prohibited group gatherings
and shortened the operating hours of bars and clubs
(if such facilities were not entirely closed) could
have significantly reduced smoking and alcohol
consumption in Hong Kong during the pandemic.
Additionally, the lower level of physical activity could
be related to the closure of public sports avenues and
restricted access to sports facilities.
The dietary habits of Hong Kong residents
have changed from the traditional Chinese diet to a
fast-paced dining experience involving convenient,
processed foods with limited diversity. Hong Kong
has a population of >7.5 million people, and 90% of
its food supply is imported from other countries.24
Woo et al11 concluded that, despite geographical
and cultural differences, traditional Chinese dietary
habits were conceptually similar to the health-promoting
Mediterranean diet. In 2001, high overall
adherence to the Mediterranean diet was observed
across all age-groups in Hong Kong, except for
younger populations and men.11 In contrast, the
present study showed that a smaller proportion
of participants in all age and sex groups had high
overall adherence to the Mediterranean diet. In this
study, intriguingly, women consistently exhibited
higher Mediterranean diet score (71%) and HKDS
(53%; P<0.005) results, compared with their male
counterparts. Moreover, the present study revealed
lower prevalences of some chronic diseases among
women: diabetes, cardiovascular disease, liver
disease, and renal disease. The contemporary diets
in modern Hong Kong and many developed regions
have low fibre content and high processed food
content; they also include food additives, refined sugar, and hydrogenated fats.25 The subtle but
consistent westernisation of dietary habits appears
to be detrimental for residents who consistently
consume these food items.
A lack of colourful vegetables and fruits may
reduce the diversity of beneficial gut microbiota,26
although leafy greens such as pak choy (Chinese
cabbage), choy sum (Chinese flowering cabbage),
and Chinese kale are staple foods in the Hong Kong
diet throughout the year. Moreover, in a review of
literature concerning exercise and gut microbial
composition, Mitchell et al27 found that exercise
alters gut microbiota; however, the direction of
apparent change has varied among studies. Increases
in butyrate-producing bacteria and faecal butyrate
concentrations, with protective anti-inflammatory
effects and the potential to enhance anti-infection
immunity, have been observed among physically
active adults.28 The mechanisms are unclear but the benefits of adopting a lifestyle with a diverse diet
and physical activity consistently create an optimal
environment for gut microbiota.
Limitations
The large sample size and random sampling design
of this territory-wide survey were strengths that
enhanced the validity of the findings. However, this
study had several limitations that should be addressed.
First, cause-and-effect relationships between the
COVID-19 pandemic and changes in lifestyle habits
could not be established because of the cross-sectional
approach. Individuals in home quarantine
during the third wave of the pandemic might have
experienced temporary changes in lifestyle habits;
a prospective observational study and longer
trend analysis are needed to facilitate long-term
comparisons. Factors other than the pandemic (eg,
mental wellness) could also have affected lifestyles
among the study population. Although the present
study utilised a random sampling strategy, non-response
and selection biases were possible because
younger segments of the Hong Kong population
did not use landlines during the study period.
Furthermore, response and social desirability biases
may have been present in this telephone survey.
Nevertheless, the high response rate and anonymous
nature of this survey may have minimised these
potential biases. Additionally, generalisation of the
study findings should be performed with caution
because the survey only included a single Chinese
population. Considering that the participants’
characteristics differed from the general population,
the findings might not be directly applicable to the
general public. Moreover, the survey was conducted
in 2020, and lifestyle habits in the general population
might have changed throughout the pandemic.
Finally, the low case numbers of some self-reported diseases, such as renal disease and cancer, may have resulted in type II error.
Conclusion
This representative population-based survey revealed that larger proportions of the general
population had unhealthy lifestyles, including dietary
habits and physical inactivity, during the COVID-19
pandemic than during pre-pandemic years. There is
an urgent need to formulate and implement effective
public health strategies at both individual and
organisational levels. The encouragement of healthy
lifestyles through evidence-based health promotion
programmes is essential. This encouragement could
be conveyed to communities through organised and
concerted efforts by the government and relevant
stakeholders. Future studies should evaluate the
effectiveness of various interventions and approaches
to achieve these important goals.
Author contributions
Concept or design: WYY Lin, MCS Wong.
Acquisition of data: WYY Lin, J Huang, Y Bai.
Analysis or interpretation of data: WYY Lin, J Huang, Y Bai.
Drafting of the manuscript: WYY Lin, MCS Wong.
Critical revision of the manuscript for important intellectual content: All authors.
Acquisition of data: WYY Lin, J Huang, Y Bai.
Analysis or interpretation of data: WYY Lin, J Huang, Y Bai.
Drafting of the manuscript: WYY Lin, MCS Wong.
Critical revision of the manuscript for important intellectual content: All authors.
All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Conflicts of interest
As editors of the journal, MCS Wong and J Huang were not involved in the peer review process. Other authors have disclosed no conflicts of interest.
Funding/support
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This research was approved by the Survey and Behavioural Research Ethics Committee of The Chinese University of Hong Kong (Ref No.: SBRE-20-099). The interviewees provided
informed consent after they were briefed on the study purpose
and being assured of the confidentiality measures in place.
References
1. World Health Organization. WHO Coronavirus Disease
(COVID-19) Dashboard. Available from: https://covid19.who.int/. Accessed 19 Jan 2024.
2. Centre for Health Protection, Department of Health,
Hong Kong SAR Government. Situation of COVID-19 (23
January 2020 to 29 January 2023). 2023 July 27. Available
from: https://www.chp.gov.hk/files/pdf/local_situation_covid19_en.pdf. Accessed 2 Feb 2024.
3. Chief Executive’s Office, Hong Kong SAR Government.
Fighting the virus for six months battling another wave of the epidemic together. 2020 Jul 25. Available from: https://www.ceo.gov.hk/archive/5-term/eng/pdf/article20200725.pdf. Accessed 6 Apr 2022.
4. Mattioli AV, Sciomer S, Cocchi C, Maffei S, Gallina S.
Quarantine during COVID-19 outbreak: changes in diet
and physical activity increase the risk of cardiovascular
disease. Nutr Metab Cardiovasc Dis 2020;30:1409-17. Crossref
5. Bin Mahfoz TM, Shaik RA, Ahmad MS, Alzerwi NA,
Almutairi R. A nationwide survey to assess COVID-19’s
impact on health and lifestyle in Saudi Arabia. Eur Rev
Med Pharmacol Sci 2022;26:4092-101. Crossref
6. Mitchell JJ, Bu F, Fancourt D, Steptoe A, Bone JK.
Longitudinal associations between physical activity and
other health behaviours during the COVID-19 pandemic:
a fixed effects analysis. Sci Rep 2022;12:15956. Crossref
7. Wang JX, Huang J, Cheung CS, Wong WN, Cheung NT,
Wong MC. Adoption of an electronic patient record
sharing pilot project: cross-sectional survey. J Med Internet
Res 2020;22:e13761. Crossref
8. de Groot LC, van Staveren WA, Burema J. Survival beyond age 70 in relation to diet. Nutr Rev 1996;54:211-2. Crossref
9. Fung TT, Rexrode KM, Mantzoros CS, Manson JE,
Willett WC, Hu FB. Mediterranean diet and incidence of
and mortality from coronary heart disease and stroke in
women. Circulation 2009;119:1093-100. Crossref
10. Bamia C, Lagiou P, Buckland G, et al. Mediterranean diet
and colorectal cancer risk: results from a European cohort.
Eur J Epidemiol 2013;28:317-28. Crossref
11. Woo J, Woo KS, Leung SS, et al. The Mediterranean score of dietary habits in Chinese populations in four different geographical areas. Eur J Clin Nutr 2001;55:215-20. Crossref
12. Centre for Food Safety, Hong Kong SAR Government.
Nutrient and health—maintain optimal nutrient intake.
2008. Available from: https://www.cfs.gov.hk/english/multimedia/multimedia_pub/multimedia_pub_fsf_28_02.html . Accessed 30 Sep 2020. Crossref
13. Torenfält I, Dimberg L. Stroke and death — findings from a 25-year follow-up of a cohort of employed Swedish middle-aged men of the Coeur study. J Public Health 2022;30:1713-24. Crossref
14. Faury H, Courboulès C, Payen M, et al. Medical features of
COVID-19 and influenza infection: a comparative study in
Paris, France. J Infect 2021;82:e36-9. Crossref
15. Center for Health Protection, Department of Health, Hong
Kong SAR Government. Non-communicable Disease
Branch. Publications. Available from: https://www.chp.gov.hk/en/resources/29/100057.html. Accessed 31 Jan 2024.
16. Centre for Health Protection, Department of Health,
Hong Kong SAR Government. Report of Health Behaviour Survey 2018/19. Available from: https://www.chp.gov.hk/files/pdf/report_of_health_behaviour_survey_2018_en.pdf. Accessed 29 Jan 2021.
17. World Health Organization. Global health risks: mortality
and burden of disease attributable to selected major
risks. 2009. Available from: https://apps.who.int/iris/handle/10665/44203. Accessed 29 Jan 2021.
18. World Health Organization. Physical activity. 2022.
Available from: https://www.who.int/news-room/fact-sheets/detail/physical-activity. Accessed 22 Jan 2024.
19. Hospital Authority. Overview of Hong Kong Cancer
Statistics of 2018. 2020. Available from: https://www3.ha.org.hk/cancereg/pdf/overview/Overview%20of%20HK%20Cancer%20Stat%202018.pdf . Accessed 30 Sep 2020.
20. Micha R, Khatibzadeh S, Shi P, et al. Global, regional and
national consumption of major food groups in 1990 and
2010: a systematic analysis including 266 country-specific
nutrition surveys worldwide. BMJ Open 2015;5:e008705. Crossref
21. World Health Organization. Obesity and overweight. 2021.
Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 23 Jun 2021.
22. Nguyen TH, Vu DC. Food delivery service during social
distancing: proactively preventing or potentially spreading
coronavirus disease-2019? Disaster Med Public Health
Prep 2020;14:e9-10. Crossref
23. Wang J, Yeoh EK, Yung TK, et al. Change in eating habits
and physical activities before and during the COVID-19
pandemic in Hong Kong: a cross-sectional study via
random telephone survey. J Int Soc Sports Nutr 2021;18:33. Crossref
24. Research Office, Legislative Council Secretariat. Fact sheet:
regulation of imported food in Hong Kong. 2016. Available
from: https://www.legco.gov.hk/research-publications/english/1516fsc14-regulation-of-imported-food-in-hong-kong-20160226-e.pdf. Accessed 22 Jan 2024.
25. Jew S, AbuMweis SS, Jones PJ. Evolution of the human
diet: linking our ancestral diet to modern functional foods
as a means of chronic disease prevention. J Med Food
2009;12:925-34. Crossref
26. Garcia-Mantrana I, Selma-Royo M, Alcantara C,
Collado MC. Shifts on gut microbiota associated to
Mediterranean diet adherence and specific dietary intakes
on general adult population. Front Microbiol 2018;9:890. Crossref
27. Mitchell CM, Davy BM, Hulver MW, Neilson AP,
Bennett BJ, Davy KP. Does exercise alter gut microbial
composition? a systematic review. Med Sci Sports Exerc
2019;51:160-7. Crossref
28. Allen JM, Mailing LJ, Niemiro GM, et al. Exercise alters
gut microbiota composition and function in lean and obese
humans. Med Sci Sports Exerc 2018;50:747-57. Crossref