DOI: 10.12809/hkmj187207
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
LETTER TO THE EDITOR
Pleural adenosine deaminase cut-off value for the
diagnosis of tuberculous pleural effusion using the Diazyme assay
Aurélie Servonnet, PharmD1; Christine
Frederic1; Francisca Fargeau1; Hervé Delacour,
PharmD2,3
1 French Armed Forces Biomedical
Research Institute, B.P. 73 - 91223 Brétigny-sur-Orge Cedex, France
2 Bégin Military Teaching Hospital,
Fédération des Laboratoires, 69 Avenue de Paris - 94163 Saint-Mandé Cedex,
France
3 Val-de-Grâce Military School, 1 Place
Alphonse Laveran - 75230 Paris Cedex 05, France
Corresponding author: Prof Hervé Delacour (herve.delacour@intradef.gouv.fr)
 Full
paper in PDF
Full
paper in PDF
To the Editor—We read with interest the
article by Chang et al.1 In the
diagnosis of tuberculous pleural effusion (TBPE), they established that
26.5 U/L is the optimal cut-off value for pleural fluid adenosine
deaminase activity when using the Diazyme assay (Diazyme Laboratories, San
Diego [CA], United States) on the UniCel DxC 800 Synchron Clinical System
(Beckman Coulter, Brea [CA], United States). The Diazyme assay can be used
on various analytical systems. Therefore, one can ask the question: does
the cut-off value differ according to the analytical system? The following
two facts can provide an answer.
First, a cut-off value between 25 and 30 U/L has
been previously recommended for TBPE diagnosis (ie, an interval including
the cut-off value proposed by Chang et al1)
if the Diazyme assay is used on the Cobas 6000 system (Roche Diagnostics,
Meylan, France).2
Second, we have compared the results obtained from
using the Diazyme assay on two analytical systems: Cobas 6000 (Roche
Diagnostics) and Advia 1800 (Siemens Healthcare Diagnostics, Saint Denis,
France) by parallel-testing 79 anonymous pleural fluid samples from
different French hospitals. We observed a good correlation between the two
analytical systems (r2=0.88; t test for
correlation coefficient, P<0.001), even though bias was observed (~16
%). After using the cut-off value proposed by Chang et al,1 we observed only one misclassification between the two
analytical systems (Fig).
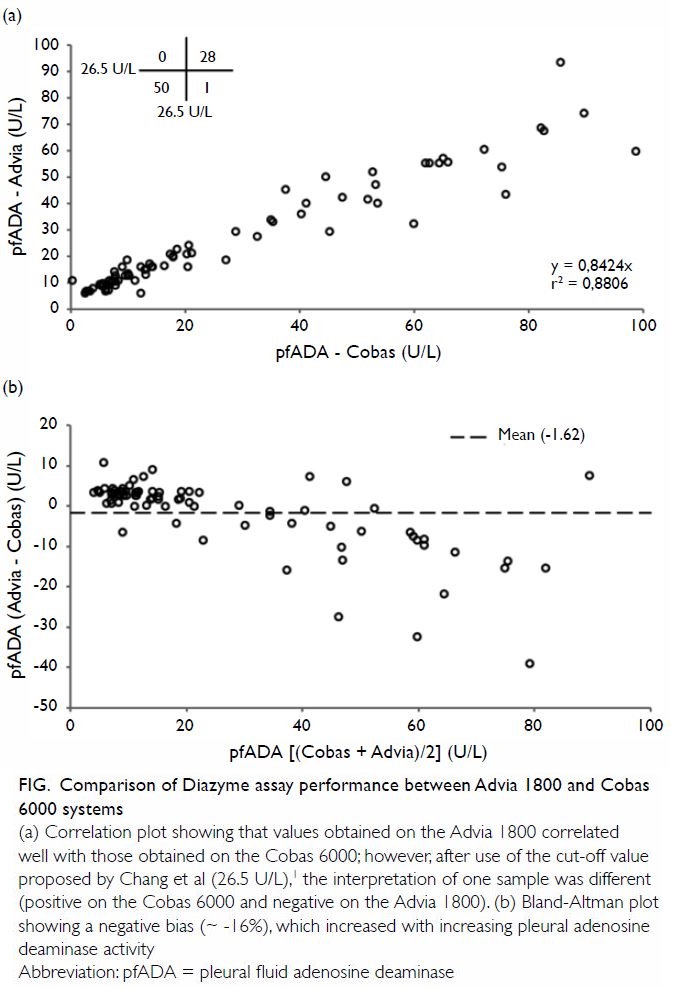
Figure. Comparison of Diazyme assay performance between Advia 1800 and Cobas 6000 systems
(a) Correlation plot showing that values obtained on the Advia 1800 correlated well with those obtained on the Cobas 6000; however, after use of the cut-off value proposed by Chang et al (26.5 U/L),1 the interpretation of one sample was different (positive on the Cobas 6000 and negative on the Advia 1800). (b) Bland-Altman plot showing a negative bias (~ -16%), which increased with increasing pleural adenosine deaminase activity
In conclusion, we consider the cut-off value
proposed by Chang et al1 for TBPE
diagnosis to be appropriate on whichever analytical system the Diazyme
assay is used.
Declaration
The authors have no conflicts of interest to
disclose.
References
1. Chang KC, Chan MC, Leung WM, et al.
Optimising the utility of pleural fluid adenosine deaminase for the
diagnosis of adult tuberculous pleural effusion in Hong Kong. Hong Kong
Med J 2018;24:38-47. Crossref
2. Delacour H, Sauvanet C, Ceppa F, Burnat
P. Analytical performances of the Diazyme ADA assay on the Cobas®
6000 system. Clin Biochem 2010;43:1468-71. Crossref