Hong
Kong Med J 2018 Apr;24(2):206.e3–4
DOI: 10.12809/hkmj166198
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Characteristic imaging features of clonorchiasis
WK Lo, MB, BS, FRCR1; SM Yu, FRCR,
FHKAM (Radiology)2; James CS Chan, FRCR, FHKAM (Radiology)2
1 Department of Diagnostic and
Interventional Radiology, Kwong Wah Hospital, Yaumatei, Hong Kong
2 Department of Radiology and Organ
Imaging, United Christian Hospital, Kwun Tong, Hong Kong
Corresponding author: Dr WK Lo (waikglo@gmail.com)
 Full
paper in PDF
Full
paper in PDF
A 43-year-old Chinese man presented to United
Christian Hospital, Hong Kong, in January 2016, with a 2-year history of
vague right upper quadrant pain. Blood test results were unremarkable
except for an episode of transient eosinophilia. Ultrasonography showed
mildly dilated intrahepatic ducts. Magnetic resonance
cholangiopancreatography showed diffuse and uniform mild dilatation of
peripheral intrahepatic bile ducts (Fig 1) consistent with the ‘too many intrahepatic
ducts’ sign (Fig 2). Notably, there was no central extrahepatic
bile duct dilatation. Subsequently requested stool microscopy was positive
for Clonorchis sinensis ova. The patient was given a course of
praziquantel.
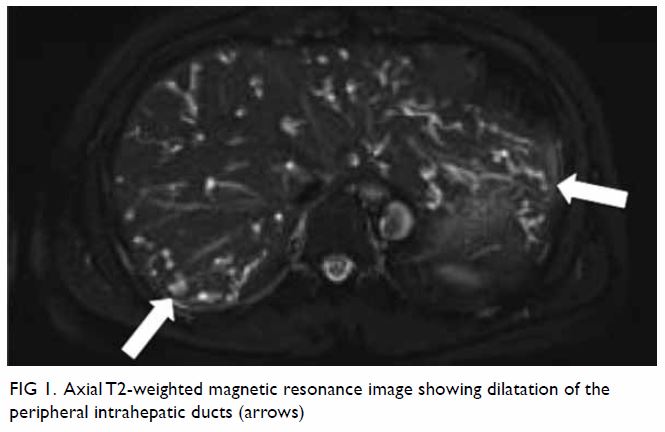
Figure 1. Axial T2-weighted magnetic resonance image showing dilatation of the peripheral intrahepatic ducts (arrows)
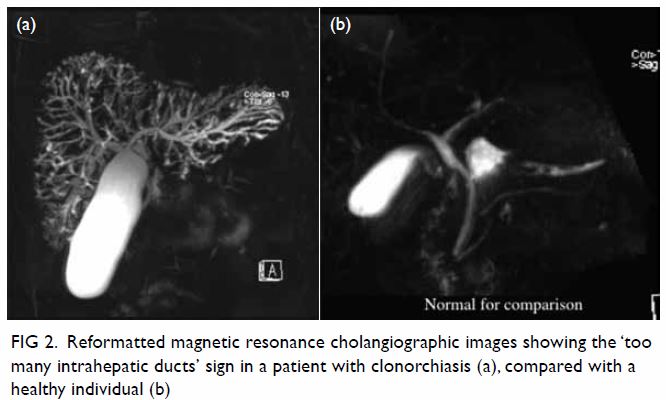
Figure 2. Reformatted magnetic resonance cholangiographic images showing the ‘too many intrahepatic ducts’ sign in a patient with clonorchiasis (a), compared with a healthy individual (b)
Clonorchiasis is a foodborne zoonosis caused by
consumption of raw or undercooked freshwater fish infested by the liver
fluke C sinensis. C sinensis larvae penetrate the scales of
freshwater fish and encyst in subcutaneous tissues. Cysts, when consumed
by a definitive host, hatch in the intestine and migrate to the biliary
tree, where the adult flukes establish residence. Clonorchiasis is endemic
in many parts of Asia, including China, Korea, and Vietnam.1 Clonorchiasis and its complications are not commonly
seen in affluent populations, such as those in Hong Kong. However, the
increasing mobility of people around the region means that clinicians
should be vigilant of the condition and alert to its symptoms. Knowledge
of the characteristic imaging features of clonorchiasis would prompt stool
microscopy and allow early diagnosis.
Within the biliary tree, adult C sinensis
flukes reside in small- or medium-sized peripheral intrahepatic ducts. The
organisms cause dilatation of the intrahepatic ducts. In heavy
infestations, the extrahepatic ducts, the gallbladder, or even the
pancreatic duct can also be involved. The dilated peripheral ducts can be
visualised by direct cholangiography, or to a better extent by magnetic
resonance cholangiopancreatography (owing to the independence of rate and
volume of the contrast injection), as the ‘too many intrahepatic ducts’
sign.2 Occasionally, linear or
elliptical filling defects representing the flukes can be seen.3
Light infestations with C sinensis can be
asymptomatic. Heavier infestations can result in fever, jaundice, right
upper quadrant pain, and eosinophilia. Untreated, chronic clonorchiasis
induces chronic inflammation of the bile ducts. Recurrent pyogenic
cholangitis, cholelithiasis, pancreatitis, and cholangiocarcinoma are the
main complications.4
Infestations are diagnosed by observation of C
sinensis ova during stool microscopy. Immunological and molecular
techniques of diagnosis are still at the experimental stage.1 Praziquantel is the only drug treatment for
clonorchiasis that is recommended by the World Health Organization.1
In summary, clinicians in Asia should be vigilant
of clonorchiasis. In modern clinical practice, magnetic resonance
cholangiopancreatography is often requested for non-invasive evaluation of
the biliary tree. Knowledge and recognition of the characteristic imaging
features of clonorchiasis would prompt timely investigation by stool
microscopy. Early diagnosis and treatment of clonorchiasis can prevent
complications such as recurrent pyogenic cholangitis and
cholangiocarcinoma.
Declaration
The authors have no conflicts of interest to
disclose.
References
1. World Health Organization. Foodborne
trematode infections—clonorchiasis. Available from:
http://www.who.int/foodborne_trematode_infections/clonorchiasis/en/.
Accessed on 27 Nov 2016.
2. Choi D, Hong ST. Imaging diagnosis of
clonorchiasis. Korean J Parasitol 2007;45:77. Crossref
3. Lim JH. Radiologic findings of
clonorchiasis. AJR Am J Roentgenol 1990;155:1001-8. Crossref
4. Choi BI, Han JK, Hong ST, Lee KH.
Clonorchiasis and cholangiocarcinoma: etiologic relationship and imaging
diagnosis. Clin Microbiol Rev 2004;17:540-52. Crossref