© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
REMINISCENCE: ARTEFACTS FROM THE HONG KONG MUSEUM OF MEDICAL SCIENCES
Jamshidi needle
Raymond Liang, MD, FHKAM (Medicine)
Member, Education and Research Committee, Hong Kong Museum of Medical Sciences Society
 Full paper in PDF
Full paper in PDF
The Jamshidi needle is the standard instrument used
for bone marrow biopsy. Bone marrow examination
is commonly performed for the diagnosis and
management of blood diseases. It usually involves
both a marrow blood aspiration and a marrow
trephine biopsy. Interpretation of a bone marrow
specimen is in the context of a good clinical history,
physical examination, and the results of at least a
complete blood count and peripheral blood smear
examination. Depending on the diagnosis, in addition
to conventional morphological examination under
light microscopy, the marrow specimen may be
sent for immunophenotyping, cytogenetic analysis,
or molecular genetic studies. For selected cases,
microbiological tests, especially viral studies using
immunological or molecular genetic techniques,
may help establish a diagnosis.1
A dry tap may occasionally be encountered
during marrow aspiration. The operator is unable
to aspirate marrow blood from the biopsy site. This
may be due to myelofibrosis or heavy malignant
marrow infiltration. Under such circumstances, a
biopsy imprint may be prepared from the trephine
specimen on a clean glass slide. This allows optimal
cytological examination of marrow cells by the
haematopathologist.
Indications for bone marrow examination
include undiagnosed anaemia, leukopaenia,
thrombocytopaenia or pancytopaenia, and to investigate the cause of elevated blood counts
including polycythaemia, leukocytosis, and
thrombocytosis. A bone marrow evaluation is
essential for the diagnosis of leukaemia and plasma
cell myeloma, and for staging of lymphoma. For
the latter, bilateral marrow aspiration and trephine
biopsy are often recommended although studies
show that unilateral biopsy is usually adequate if
the length of the trephine biopsy specimen exceeds
20 mm. Bone marrow examination may also be
performed in cases of unexplained splenomegaly.
The posterior superior iliac crest and spine are
the chosen sites for marrow aspiration and trephine
biopsy. The procedure is usually performed under
local anaesthesia. Other premedications or sedation
including anxiolytics or opiates are not usually
necessary for adults.
The patient is advised to lie supine for at least
15 minutes following the procedure and inspected
for bleeding before discharge. Paracetamol may be
given to control pain. The patient should be advised
that there may be slight tenderness or numbness
around the puncture wound for a few days and to
contact the clinic if there is increasing tenderness,
swelling, or bleeding.2 The wound should be kept dry
and heavy exercise should be avoided. Complications
including bleeding and infection are rare.
Trepanning of bone has a very long history.3
There is evidence that the procedure was once performed on the bones of the skull to treat
headache and mental illness. Obtaining a bone
marrow specimen for diagnostic purposes was first
performed by Pianese in 1903 in Italy, by puncturing
the epiphysis of a femur. Over the years, different
needles have been designed for similar purposes.
The ultimate instrument, the Jamshidi needle, was
designed and patented in 1971. It was named after the
inventor Dr Khosrow Jamshidi, an Iranian physician.3
The original Jamshidi needle was made of
stainless steel, including the handle, and was reusable
(Fig). It can be used for both marrow blood aspiration
and trephine biopsy.3 It is a long hollow needle with a
tapering sharp cutting end and a handle at the other
end, with a solid stylet inside the needle. A 20-mL
syringe with no luer lock is usually used for marrow
aspiration. The unique feature of this needle is that
the interior diameter of its distal end tapers radially
towards the cutting tip. This allows the trephine specimen to enter freely into the lumen and hence
avoids crushing of the marrow tissue. As the needle
has a tapering end, it is important to use the provided
guidewire to push out the trephine specimen away
from the sharp end, to avoid compressing marrow
cells.
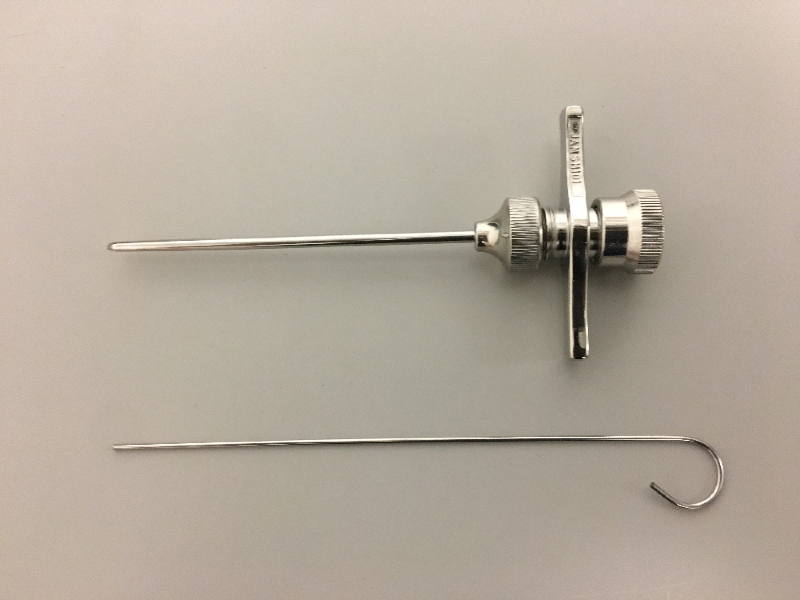
Figure. Jamshidi needle with stylet in situ (above) and the guidewire (below) used for detaching the marrow specimen from its lumen
Specimen was donated to the Hong Kong Museum of Medical Sciences in 2016 by the Department of Medicine, The University of Hong Kong
A Jamshidi needle is now the standard
instrument used by haematologists worldwide for
marrow aspiration and trephine biopsy. It must be
sterilised before use and sharpened periodically.
The original reusable Jamshidi needle, however, has
now almost completely been replaced by disposable
needles although its basic design is unchanged. This
ensures sharpness and sterility, and a higher yield
with less pain to patients.
Modification of the marrow biopsy technique
is advocated only in the most difficult cases and
includes use of an electric drill and guidance by
computed tomography.
References
1. Zehnder JL. Bone marrow aspiration and biopsy: indications and technique. 2016 May. Available from: http://www.uptodate.com/contents/bone-marrow-aspiration-and-biopsy-indications-and-technique. Accessed Jun 2017.
2. Le Dieu R, Luckit J, Sundarasun M. Complications of trephine biopsy. Br J Haematol 2003;121:822. Crossref
3. Parapia LA. Trepanning or trephines: a history of bone marrow biopsy. Br J Haematol 2007;139:14-9. Crossref