DOI: 10.12809/hkmj154644
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
CASE REPORT
Self-inflicted transorbital brain injury by
chopsticks in a patient with acute psychosis
YC Lee, MB, ChB, MRCP1; HH Kwan, MB, BS, MRCP2; T Wong, MB, ChB, FRCR1; NY Pan, FRCR, FHKAM (Radiology)1; HY Lai, FRCR, FHKAM (Radiology)1; KF Ma, FRCR, FHKAM (Radiology)1
1 Department of Radiology, Princess Margaret Hospital, Laichikok, Hong Kong
2 Division of Neurology, Department of Medicine, Princess Margaret Hospital, Laichikok, Hong Kong
Corresponding author: Dr YC Lee (lyc713@ha.org.hk)
All authors contributed equally to this case report.
 Full
paper in PDF
Full
paper in PDF
Case report
A 56-year-old man was admitted from the emergency
department with acute onset of psychotic symptoms
and suicidal ideation in January 2015. While under
observation in the emergency medical ward, he
self-inflicted orbital injuries with two plastic
chopsticks. The chopsticks were pulled out by the
patient. Further injury was immediately stopped
by the attending physician. Urgent computed
tomographic (CT) brain showed two almost-parallel
haemorrhagic penetration tracts extending
posterosuperiorly from bilateral inferior frontal
lobes (Fig a, b) to involve the caudate and lentiform nuclei (Fig c), barely missing the internal capsules.
Reformatted images revealed defects in both orbital
roofs (Fig d), indicating fractures. The trajectories
of penetration were recreated by extrapolating the
linear haematomas on a workstation (Fig e). No
retained foreign body was detected. Subsequent
digital subtraction angiogram and CT angiogram
did not demonstrate any vascular injury. The patient
was clinically and neurologically stable throughout
the admission, and was managed conservatively
without any neurosurgical intervention. The
patient’s psychiatric symptoms gradually subsided
after starting antipsychotic medication and he was
discharged without significant neurological deficit.
Only mild cogwheel rigidity in the upper limbs was
noted during neurological follow-up.
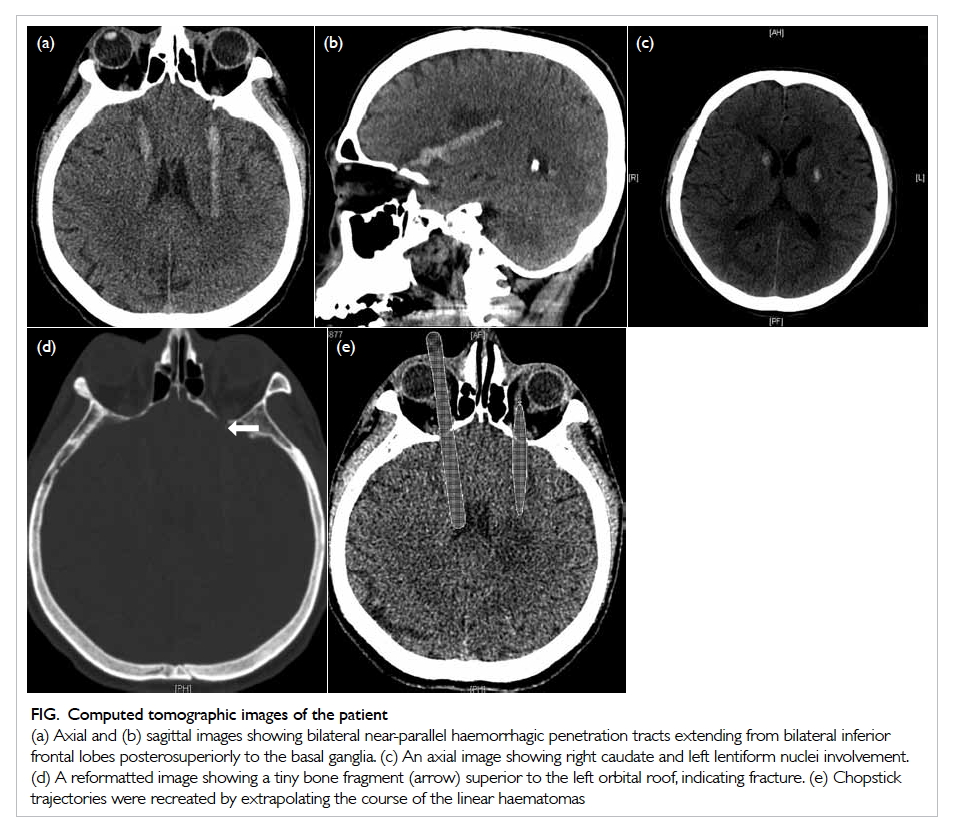
Figure. Computed tomographic images of the patient
(a) Axial and (b) sagittal images showing bilateral near-parallel haemorrhagic penetration tracts extending from bilateral inferior frontal lobes posterosuperiorly to the basal ganglia. (c) An axial image showing right caudate and left lentiform nuclei involvement. (d) A reformatted image showing a tiny bone fragment (arrow) superior to the left orbital roof, indicating fracture. (e) Chopstick trajectories were recreated by extrapolating the course of the linear haematomas
Discussion
There have been a few case reports of self-inflicted
penetrating brain injury in patients with psychiatric
symptoms. The methods of injury were often bizarre
and associated with a high mortality rate.1
Transorbital penetrating brain injury is rare but
accounts for nearly one quarter of penetrating head
injuries in adults, and one half of those in children.2
Penetrating objects such as wood,3 chopsticks,4 pens and pencils2 have been commonly implicated.
The orbit is shaped like a horizontal pyramid.
This special anatomy often directs the penetrating
object towards the apex and into the brain through
three common sites.2 The most common pathway is
through the orbital roof, as in our case. This causes
frontal lobe contusion or laceration and may injure
the anterior cerebral arteries. The next most common
path is via the superior orbital fissure in which the
cavernous sinus, brainstem, and cranial nerves can
be injured. Penetration through the optical canal
is rare.5 The penetrating object is directed into the
suprasellar cistern near the optic nerve and internal
carotid artery.6 7
Neurological signs and symptoms may initially
be absent even when both intracranial haematoma
and foreign body are present, but a patient who is
conscious on presentation can deteriorate rapidly
and therefore neurological surveillance is needed.3 7 A high degree of suspicion is required especially
when handling psychiatric patients because injuries
can be subtle and initially occult.7
Of note, CT is the initial investigation to
delineate the extent of injury, determine the presence
of retained foreign bodies, and plan subsequent
surgery. Digital subtraction angiogram or CT
angiogram is helpful when there is a suggestion of
vascular injury, either by the location and trajectory
of the foreign body or by evidence of haematoma on
initial CT scan.2
The patient in this case report was fortunate
because the trajectories of both penetration tracts
narrowly missed the internal capsules, preventing
major neurological deficit. Chung et al8 reported that
small haematomas involving caudate or lentiform
nuclei cause only mild-to-moderate or even no
motor and sensory deficit, as in our case. Injury to the
caudate and lentiform nuclei, however, may explain
the late-onset cogwheel rigidity of upper limbs in our
patient. This case also illustrates that the apparent
severity of cerebral trauma on CT may not correlate
with a patient’s initial degree of neurological deficit.
Close follow-up in an out-patient clinic is required
to detect any subtle late-onset neurological signs.
Declaration
All authors have disclosed no conflicts of interest.
References
1. Greene KA, Dickman CA, Smith KA, Kinder EJ,
Zabramski JM. Self-inflicted orbital and intracranial
injury with a retained foreign body, associated with
psychotic depression: case report and review. Surg Neurol
1993;40:499-503.
Crossref
2. Schreckinger M, Orringer D, Thompson BG, La Marca
F, Sagher O. Transorbital penetrating injury: case series,
review of the literature, and proposed management
algorithm. J Neurosurg 2011;114:53-61.
Crossref
3. Borkar SA, Garg K, Garg M, Sharma BS. Transorbital
penetrating cerebral injury caused by a wooden stick:
surgical nuances for removal of a foreign body lodged in
cavernous sinus. Childs Nerv Syst 2014;30:1441-4.
Crossref
4. Mitilian D, Charon B, Brunelle F, Di Rocco F. Removal of a
chopstick out of the cavernous sinus, pons, and cerebellar
vermis through the superior orbital fissure. Acta Neurochir
(Wien) 2009;151:1295-7.
Crossref
5. Matsumoto S, Hasuo K, Mizushima A, et al. Intracranial
penetrating injuries via the optic canal. AJNR Am J
Neuroradiol 1998;19:1163-5.
6. Di Roio C, Jourdan C, Mottolese C, Convert J, Artru F.
Craniocerebral injury resulting from transorbital stick
penetration in children. Childs Nerv Syst 2000;16:503-6.
Crossref
7. Turbin RE, Maxwell DN, Langer PD, et al. Patterns of
transorbital intracranial injury: a review and comparison
of occult and non-occult cases. Surv Ophthalmol
2006;51:449-60.
Crossref
8. Chung CS, Caplan LR, Yamamoto Y, et al. Striatocapsular
haemorrhage. Brain 2000;123(Pt 9):1850-62.
Crossref