Hong Kong Med J 2016 Oct;22(5):420–7 | Epub 19 Aug 2016
DOI: 10.12809/hkmj164853
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Seatbelt use by pregnant women: a survey of knowledge and practice in Hong Kong
WC Lam, MPH (CUHK), FHKAM (Obstetrics and Gynaecology)1;
William WK To, MD, FHKAM (Obstetrics and Gynaecology)1;
Edmond SK Ma, MD, FHKAM (Community Medicine)2
1 Department of Obstetrics and Gynaecology, United Christian Hospital,
Kwun Tong, Hong Kong
2 The Jockey Club School of Public Health and Primary Care, The Chinese
University of Hong Kong, Shatin, Hong Kong
Corresponding author: Dr WC Lam (lamwc2@ha.org.hk)
 Full
paper in PDF
Full
paper in PDF
Abstract
Introduction: The use of motor vehicles is common
during pregnancy. Correct seatbelt use during
pregnancy has been shown to protect both the
pregnant woman and her fetus. This survey aimed to evaluate the practices, beliefs, and knowledge of Hong Kong pregnant women of correct seatbelt use, and identify factors leading to reduced compliance and inadequate knowledge.
Methods: A self-administered survey was completed
by postpartum women in the postnatal ward at
the United Christian Hospital, Hong Kong, from
January to April 2015. Eligible surveys were available
from 495 women. The primary outcome was the
proportion of pregnant women who maintained or
reduced seatbelt use during pregnancy. Secondary
outcomes were analysed and included knowledge
of correct seatbelt use, as well as contributing factors to non-compliance
and inadequate knowledge.
Results: There was decreased compliance with
seatbelt use during pregnancy and the decrease was
in line with increasing gestation. Pregnant women’s
knowledge about seatbelt use was inadequate and
only a minority had received relevant information.
Women who held a driving licence and had a higher
education level were more likely to wear a seatbelt
before and during pregnancy. Women with tertiary
education or above knew more about seatbelt use.
Conclusions: Public health education for pregnant
women in Hong Kong about road safety is advisable,
and targeting the lower-compliant groups may be
more effective and successful.
New knowledge added by this study
- There was decreased compliance with seatbelt use by pregnant women in Hong Kong. The decrease in compliance became more pronounced as gestation increased. This may be related to lack of relevant information and misconceptions.
- As a form of public health and road traffic safety promotion, information about seatbelt use during pregnancy should be provided to pregnant women, health care workers, and all road traffic users.
Introduction
Road traffic safety is an important public health issue.
Health care professionals are usually involved in the
treatment of road traffic accident victims rather than
prevention of their occurrence or minimising the
severity of injury. Education about and promotion
of road traffic safety is important for all; pregnant
women are no exception. Safety issues relate to both
the mother and her fetus, and different information
and/or a different approach may be required. With
any kind of intervention during pregnancy, an
emphasis on the safety of the fetus may improve
compliance.
The number of pregnant drivers in Hong Kong
is unknown, but the use of motor vehicles including
private car, taxi, and public light bus is common
during pregnancy. To promote maternal seatbelt use
among the local pregnant population, information
about their beliefs is essential.
Correct seatbelt use during pregnancy has
been shown to protect both the pregnant woman and
her fetus. There is evidence that pregnant women
who do not wear a seatbelt and who are involved in a
motor vehicle accident are more likely to experience
excessive bleeding and fetal death.1 2 3 Compliance
and proper use of the seatbelt are crucial. Incorrect
placement of the seatbelt and a subsequent accident
may result in fetal death due to abruptio placentae.4
The three-point restraint (ie shoulder harness in
addition to a lap belt) provides more protection
for the fetus than a lap belt alone. Previous studies
have revealed incorrect positioning of the seatbelt
in 40% to 50% of pregnant women.5 6 Various other
studies have shown reduced seatbelt compliance
during pregnancy.7 The proportion of seatbelt use
has been reported to be around 70% to 80% before
pregnancy, but reduced by half at 20 weeks or more
of gestation.5 7 There is also evidence that pregnant
women lack information about the proper use of a
seatbelt and its role in preventing injury: only 14%
to 37% of pregnant women received advice from
health care professionals.5 6 7 8 The common reasons for
not using a seatbelt have been reported to include
discomfort, inconvenience, forgetfulness, and fear of
harming the fetus.9
In this study, the current practice and
knowledge of Hong Kong pregnant women about
seatbelt use was surveyed, and any determining
factors were identified. The results will enable public
health education and promotion to be targeted to
at-risk groups to improve road traffic safety among
local pregnant women.
Methods
Study design
This was a cross-sectional survey using a convenient
sampling carried out from January to April 2015.
A self-administered questionnaire was distributed
to postpartum women in the postnatal ward of
United Christian Hospital (UCH) in Hong Kong.
Participation in the survey was entirely voluntary.
Questionnaires were analysed if at least
50% of questions were answered, including the
main outcomes. Those from women who did not
understand the content or who did not understand
Chinese or English were excluded.
Questionnaire
The questionnaire was based on a pilot study, with
questions revised after review. It was available in
English and Chinese (traditional and simplified)
versions and was divided into four parts. The first part
included demographic and pregnancy information
and driving experience. The second part focused on
practice of seatbelt use before and during pregnancy,
any change in habit with progression of pregnancy,
and the reason(s) for non-use of a seatbelt. The third
part related to awareness and knowledge of the Road
Traffic Ordinance on seatbelt use and the correct
use of both lap and shoulder belts. Text descriptions
and diagrams of different restraint positions were
provided. The correct way is to place the lap belt
below the abdomen and the shoulder belt diagonally
across the chest. The diagram of restraint positions
were adopted from the leaflet “Protect your unborn
child in a car” by the Transport Department of
Hong Kong with permission.10 The final part asked
whether the postpartum woman had received any
advice about seatbelt use during pregnancy, the
source of information, and whether they thought
such information was useful and/or relevant.
Statistical analysis
Sample size calculation
Using the results of overseas studies as reference,
the sample size was calculated according to the
assumption that around 80% of Hong Kong pregnant
women use a seatbelt. A previous questionnaire
survey among postpartum women at a local hospital
indicated that a response rate of approximately 80%
could be expected.11 We assumed the margin of error
that could be accepted to be 4%, with a confidence
level of 95%, and using this formula: n = z2 x p x (1-p)/d2 (where p = proportion of wearing seatbelt [0.8]; d = margin of error [0.04]; and z value = 1.96), the adjusted sample size was 481.
All statistical analysis was performed using
PASW Statistics 18 (Release Version 18.0.0; SPSS
Inc, Chicago [IL], US). For categorical data, the
Chi squared test was used to compare knowledge
about seatbelt use in wearers and non-wearers. For
continuous data with a highly skewed distribution,
non-parametric test (Mann-Whitney U test for two
groups and Kruskal-Wallis H test for more than
two groups) was used to compare the knowledge of
correct seatbelt use. Knowledge score was calculated
based on the answer to questions about the Road
Traffic Ordinance on seatbelt use and the proper way
to use both the lap and shoulder belts. One point was
given for each correct answer. The critical level of
statistical significance was set at 0.05.
The relative effects of factors (age, marital
status, education level, resident status, husband’s
occupation, family monthly income, respondent’s
and husband’s driving licence holder status,
frequency of public transport use, and stage of
pregnancy) that might influence seatbelt use
during pregnancy were estimated using generalised
estimating equation (GEE). The outcome variables
were dichotomous correlated responses (eg use of
seatbelt in different gestations), and the outcome
variables were assumed to be independent. The
issue about statistical significance due to lack of
independence was corrected using GEE.
To account for the interdependence of
observations, we used robust estimates of variance
(GEE) by including each period of observation as a
cluster. For use of a seatbelt before and during each
trimester of pregnancy, since the responses were
correlated as time progressed, the GEE model with
working correlation matrix was adopted.12
Results
Demographic data
There were 769 postpartum women in the postnatal
ward during the study period. A total of 550
questionnaires were distributed by convenience and
the response rate was 91% with 501 questionnaires
returned. The remaining women (n=49, 9%)
either refused to participate or did not return the
questionnaire. Among the returned questionnaires,
six were excluded due to missing information on
the main outcomes of the survey or they were <50%
complete. At the end of the recruitment period, 495
(90%) questionnaires were valid for analysis.
The majority (93.5%) of respondents were
aged between 21 and 40 years. Only 10 (2%) were
English speakers; others (98%) spoke Cantonese
or Mandarin as their first language and completed
the Chinese questionnaire. With regard to
education level, 188 (38%) women had received
tertiary education or above, 290 (58.6%) secondary
education, and 14 (2.8%) primary education. There
was no existing information about any association
between pregnant woman or spousal occupation and
compliance with or knowledge about seatbelt use.
We therefore investigated whether occupation was
a relevant factor, for example, driver and health care
worker. Around half (n=216, 43.6%) of the women
were housewives, 57 (11.6%) were professionals, and
14 (2.8%) were medical health care workers. Among
spouses, 32 (6.5%) were drivers, two (0.4%) were
medical health care workers, and 122 (24.6%) were
professionals. Other occupations were unrelated
to transportation or health care, including clerk,
construction site worker, restaurant waiter, and
chef. Overall, 439 (88.7%) women were Hong Kong
residents, others were new immigrants or double-entry
permit holders from Mainland China. Of
the respondents, 477 (96.4%) women had attended
regular antenatal check-ups, and 215 (43.4%) were
first-time mothers.
Driving experience and mode of transport
Around half of the spouses (49.1%) but only 71 (14.3%)
women held a Hong Kong driving licence. Among
those women with a driving licence, only 16 (22.5%)
drove daily, and seven (9.9%) only at weekends.
Public transport was used daily by 300 (60.6%)
women. Among different means of public transport,
buses (53.7%) were the most commonly used but not
all seats on buses have seatbelts. In public light buses
and taxis, use of a seatbelt, if available, is mandatory:
38.6% and 15.2% of respondents used public light
buses and taxis, respectively.
Use of a seatbelt before and during pregnancy
Of the respondents, 379 (76.6%) pregnant women
reported using a seatbelt in the 6 months before
pregnancy, but compliance was reduced as pregnancy
progressed. Seatbelt use was reduced to 73.5% in the
first trimester, 70.5% in the second trimester, and
67.1% in the third trimester (Table 1). There were
26 women who changed their behaviour from not
wearing a seatbelt prior to pregnancy to wearing
one after they became pregnant. Therefore the total
number of ever seatbelt users was 405. Analysis of the
knowledge score was performed by excluding these
26 women; the result showed a similar finding and
statistical significance.
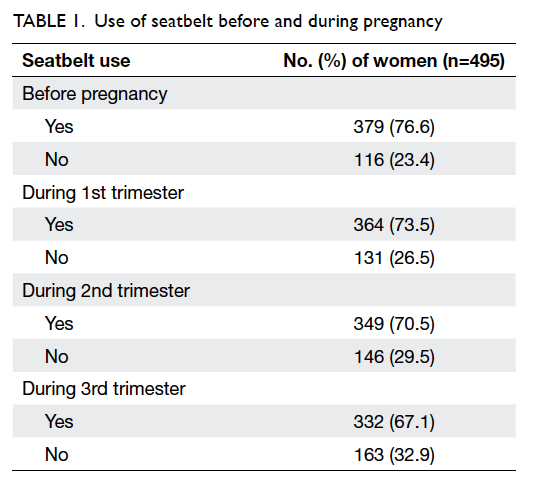
Table 1. Use of seatbelt before and during pregnancy
Reasons for not using a seatbelt during pregnancy
With regard to the reasons for not using a
seatbelt at any time during pregnancy, 156 (89.1%) of 175
women stated that the seatbelt caused discomfort,
22 (12.6%) thought seatbelts were not useful, and 79
(45.1%) worried that they would cause harm to the
fetus (Table 2). Apart from the three stated options
in the questionnaire, several respondents stated that
the travelling distance was usually short on public
light buses and the time taken to buckle up and
unfasten the seatbelt may delay other passengers.
Other women admitted to being lazy or forgetful, or
were just not in the habit of using a seatbelt. They
also found seatbelts inconvenient because those on
public transport were “not user-friendly”, “too short”,
or were “dirty” (Table 2).
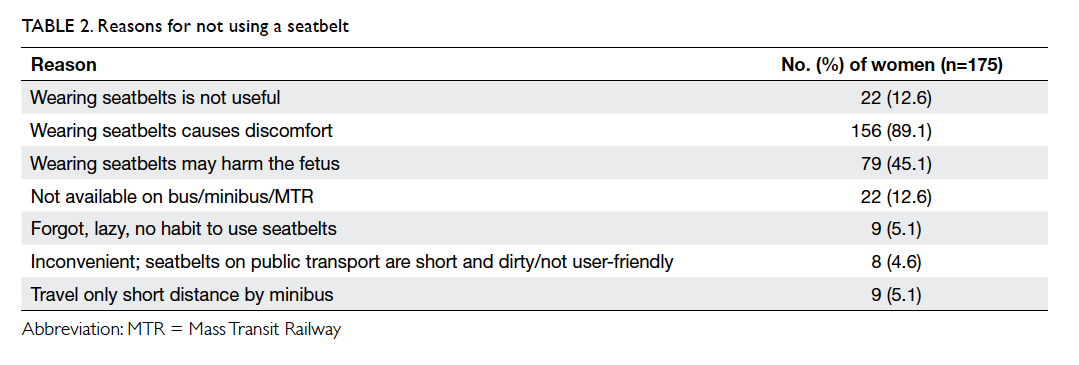
Table 2. Reasons for not using a seatbelt
Knowledge of seatbelt use during pregnancy
Of the respondents, 216 (43.6%) correctly answered
that pregnant women are not exempted from seatbelt
use according to the Road Traffic Ordinance. The
remaining 56.4% either answered wrongly or did
not know the answer. Approximately 52.7% women
correctly pointed out that appropriate use of a
seatbelt will not harm the fetus. Although around
half of the women wrongly believed that pregnant
women are exempted from seatbelt legislation or
that use of a seatbelt will harm the fetus, 358 (72.3%)
stated that pregnant women should wear a seatbelt.
When the three-point seatbelts were shown on the
diagrams, 403 (81.4%) women could identify the
correct way of wearing the seatbelt with the lap strap
placed below the bump, not over it (Table 3).
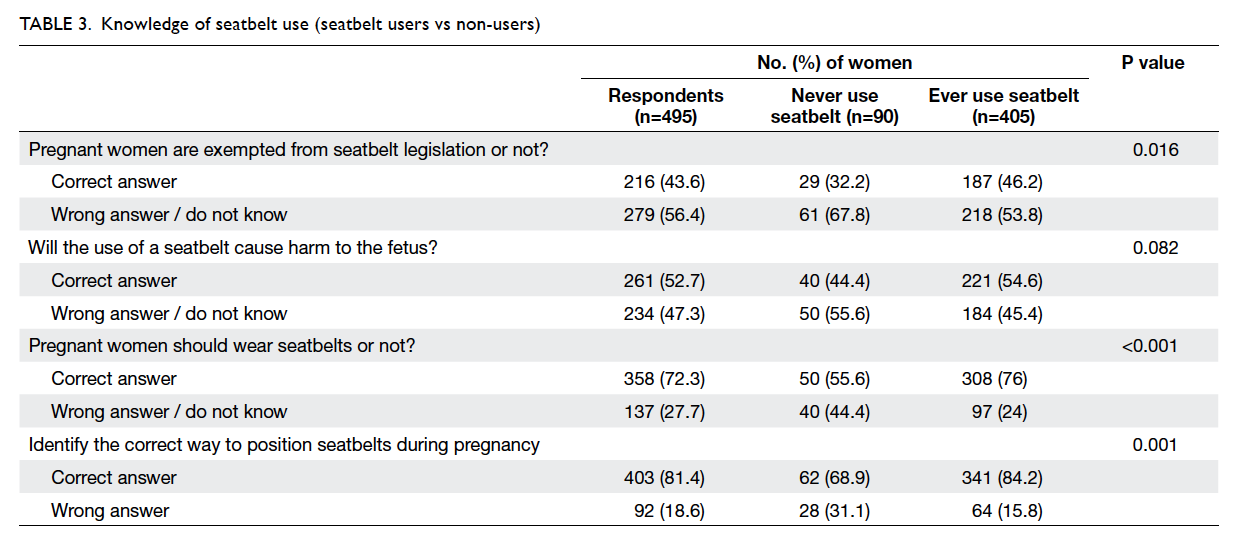
Table 3. Knowledge of seatbelt use (seatbelt users vs non-users)
Among all the respondents, 90 (18.2%)
women never wore a seatbelt, and the other 405
(81.8%) were seatbelt users either before or during
pregnancy. Comparison of responses revealed that
never wearers of a seatbelt had significantly poorer
knowledge in three of the four questions about
seatbelt use during pregnancy (P<0.05) [Table 3].
Information about seatbelt use during pregnancy
Information about seatbelt use had been received by
only 32 (6.5%) women. Among them, 13 (40.6%) had
derived the information from the internet, others from
staff of a government and private clinic, magazine,
and publications of Transport Department. Seven
(21.9%) received information from friends or family
members; one had a car accident during pregnancy
and was given relevant information by health care
workers at the Accident and Emergency Department.
Most (n=426, 86%) women expressed the view that
information about seatbelt use during pregnancy was
useful and necessary.
Factors influencing use of seatbelt during pregnancy
Among all potential factors, women who held a
driving licence (odds ratio [OR]=3.28; P=0.004) or
had a higher level of education (OR=2.13; P<0.001)
were more likely to use a seatbelt. Considering
time as another variable, as pregnancy progressed
women were significantly less likely to use a seatbelt
(OR=0.84; P<0.001) [Table 4].
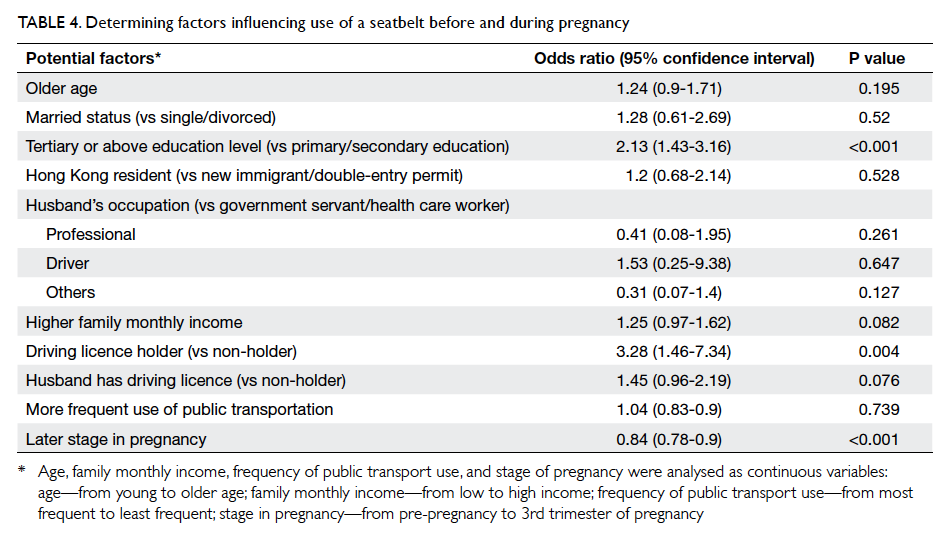
Table 4. Determining factors influencing use of a seatbelt before and during pregnancy
Factors influencing knowledge about correct seatbelt use
Women with a lower education level (P<0.001)
were less aware of the Road Traffic Ordinance on
seatbelt use, the protective effects of a seatbelt
during pregnancy, and the correct way to position
both the lap and shoulder belts (Table 5).
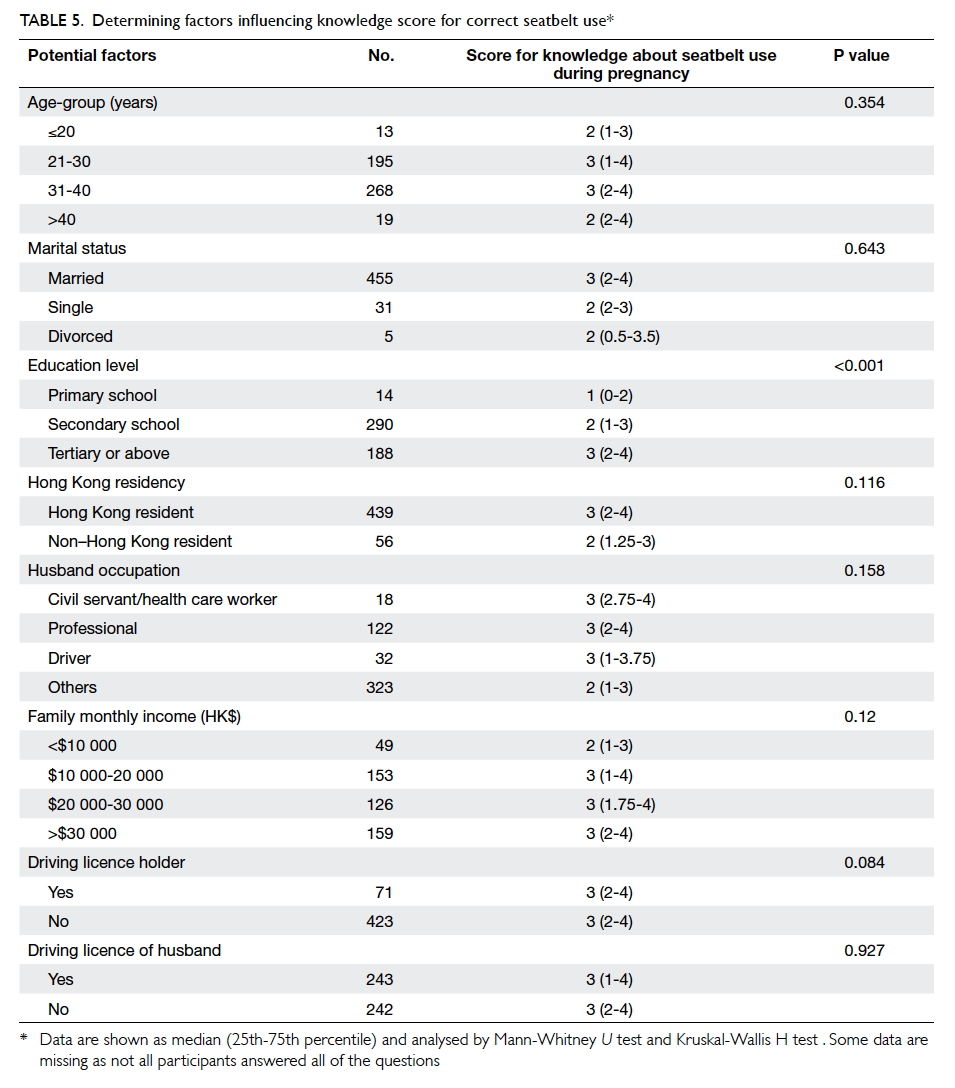
Table 5. Determining factors influencing knowledge score for correct seatbelt use
Discussion
Main findings
In this study, 76.6% of Hong Kong
pregnant women were consistent seatbelt wearers
before pregnancy; this is similar to overseas studies
which reported 70% to 80%.5 7 Compliance was
reduced during all trimesters, and decreased as
gestation progressed. Only 26 women changed their
behaviour from non-users to users after becoming
pregnant. It also demonstrated the misconception
about the effects of seatbelt use on pregnancy and
the fetus. Pregnant women’s knowledge about seatbelt use
was inadequate and only a minority had
received relevant information. Women who held
a driving licence or had a higher education level
were more likely to wear a seatbelt before and during
pregnancy. Women with a tertiary education or
above were more knowledgeable about seatbelt use.
Strengths and limitations
As far as we know, this is the first survey in Hong Kong
of the knowledge of pregnant women about seatbelt
use and their associated practice, with a reasonably
high response rate. One limitation of the study was
that the questionnaire was not validated and there
were overlapping categories for numerical variables.
Results and experience in this study can serve to
revise the questions for a future study with improved
validity and reliability. During the study period, 769
postpartum women stayed in the postnatal ward and
495 (64%) completed questionnaires were collected.
The proportion included was relatively high, but
still the method of convenient sampling may have
affected the representativeness of the sampled
subjects. Moreover this was a single-centre survey
in the obstetric unit of a district hospital. The UCH
provides obstetric services to the population in the
Kowloon East region. The geographical location of a
clinic could dictate the mode of travelling to attend
antenatal hospital appointments. Although taxis and
public light buses are the usual mode of transport,
some women may have taken the bus or Mass Transit
Railway, and these do not require use of a
seatbelt. Furthermore, the delivery rate at UCH was
less than 10% of the total deliveries in Hong Kong,
therefore the results may not be applicable to other
clusters with patients of different education levels,
driving experience, and transportation habits.
In addition, those who were unable to read or
understand Chinese or English were excluded. These
were usually illiterate or non–Hong Kong residents,
and may be the group with the lowest compliance and poorest knowledge about seatbelt use.
There were 49 women who refused to participate
and six who did not complete the questionnaire; this
10% also introduced inaccuracy and bias in our data.
Reporting bias is another concern. Discrepancies
between observed and self-reported seatbelt use
were found in a previous study.13 Anonymity of the
questionnaires might have minimised reporting
bias. Although all demographic variables included
in the questionnaire were analysed, there were other
potential confounders that might have affected the
knowledge score and the use of a seatbelt during
pregnancy. These were not investigated and hence
not adequately adjusted in the knowledge score
analysis or in the GEE model, for example prior
traffic accidents in the respondents and their family
members, risk-taking behaviours such as smoking,
alcohol drinking, and drug use. Finally, multivariate
instead of univariate analysis of the factors affecting
knowledge score could be performed to investigate
the relationship among different variables.
Interpretation
Prevention plays a major role in ensuring maternal
and fetal survival in road traffic accidents. Motor
vehicle crashes are responsible for severe maternal
injury and fetal loss. Despite existing knowledge
about the protective effects of wearing a seatbelt,
pregnant women remain poorly compliant. This
was confirmed in this local survey and in overseas
studies.14 15
In the Report on Confidential Enquiries into
Maternal Deaths in the United Kingdom 1994-1996
published by the Royal College of Obstetricians
and Gynaecologists, 13 pregnant women died as a
result of road traffic accidents. One of the victims
did not use a seatbelt and was forcibly ejected from
the vehicle.16 Ten years later, in a more recent Report
on Confidential Enquiries into Maternal Deaths in
the United Kingdom 2006-2008,17 there were 17
pregnant women who died as a result of road traffic
accidents. A specific recommendation was made in
the report: “All women should be advised to wear a
3-point seat belt throughout pregnancy, with the lap
strap placed as low as possible beneath the ‘bump’
lying across the thighs and the diagonal shoulder
strap above the ‘bump’ lying between the breasts.
The seat belt should be adjusted to fit as snugly and
comfortably as possible, and if necessary the seat
should be adjusted”.17
According to the Road Traffic Ordinance
in Hong Kong, drivers and passengers must wear
seatbelts where provided. The exceptions are when
reversing a vehicle, making a three-point turn,
manoeuvring in and out of a parking place, and
those who have a medical certificate and have been
granted an exemption on medical grounds by the
Commissioner for Transport.18 According to a report
of the Transport Department of Hong Kong, the total
number of road traffic accidents was 14 436 in 2003.
In 2013, the number rose to 16 089. The number
of pregnant women involved or injured in road
traffic accidents is unknown.19 The Hong Kong SAR
Government revises seatbelt legislation regularly to
enhance road safety. Since 1 January 2001, passengers
have been required to wear a seatbelt, if available,
in the rear of taxis as well as in the front. Since 1
August 2004, passengers on public light buses have
also been required to wear a seatbelt where one is
fitted.20 21 Stickers were put inside buses and taxis to remind passengers of their responsibility to wear a
seatbelt and to give clear instructions on the correct
way to wear it. Nonetheless, the requirement to use
a seatbelt and its protective effects were not well
recognised among the respondents in this survey.
This may be due to the lack of information provision
as only 6.5% of women had received information
related to seatbelt use in pregnancy.
In this study, those with a lower education
level had poorer knowledge about seatbelt use in
pregnancy. Effective public education should target
these women. Using diagrams as instruction can
be simple and direct so that those with a lower
education level or who only use public transportation
occasionally can easily understand and follow the
advice. In the past, leaflets or stickers about seatbelt
use were widely seen, especially after introduction
of the new legislation, but those specifically targeted
to the pregnant population were not common.
Maternal child health centres and antenatal clinics
of government hospitals are ideal places to distribute
educational material. Television announcements
may also convey the message effectively, not only
to pregnant women, but to all road traffic users. It
is also a good opportunity to inform drivers and
other passengers so that they can help pregnant
women as well as the elderly and disabled who use
public transport. Regular spot-checks on public
transport and law enforcement may also encourage
compliance with seatbelt use. The majority of
doctors and midwives give advice about seatbelt
use only if asked. This survey demonstrated that the
proportion of pregnant women who received seatbelt
information was very small. It is recommended that
written instructions and advice should be available
from well-informed health care professionals, and
pregnant women should always be encouraged to
wear a correctly positioned seatbelt. Obstetricians,
midwives, and general practitioners play an
important role in disseminating information. A study
in Ireland showed that 75% of general practitioners
believed women should wear seatbelts in the third
trimester, although only 30% provided regular advice
and fewer than 50% indicated that they were aware
of the correct advice to give.22
Conclusions
This study demonstrated decreased compliance
with seatbelt use during pregnancy that continued
to decrease as pregnancy progressed. Women with
a lower education level or without a driving licence
were less likely to use a seatbelt during pregnancy.
The former were also less aware of the Road
Traffic Ordinance on seatbelt use and the correct
way to position both the lap and shoulder belts.
Only a minority of pregnant women had received
information about seatbelt use. Future studies to
assess the knowledge of Hong Kong health care
workers about use of seatbelts in pregnancy may
enhance the awareness and involvement of medical
professionals in educating pregnant women on this
issue. Publicity and education about road safety
by health care providers and the government are
advised, and targeting the lower compliant groups
may be more effective and successful.
Acknowledgements
The authors gratefully acknowledge Mr Edward
Choi for his valuable statistical advice, the staff in
the postnatal ward of UCH for helping to collect
the questionnaires, and the Transport Department
of Hong Kong for permission to use the diagram of
restraint positions adopted from the leaflet “Protect
your unborn child in a car” on the questionnaires.
Declaration
All authors have disclosed no conflicts of interest.
References
1. Hyde LK, Cook LJ, Olson LM, Weiss HB, Dean JM. Effect
of motor vehicle crashes on adverse fetal outcomes. Obstet
Gynecol 2003;102:279-86. Crossref
2. Wolf ME, Alexander BH, Rivara FP, Hickok DE, Maier
RV, Starzyk PM. A retrospective cohort study of seatbelt
use and pregnancy outcome after a motor vehicle crash. J
Trauma 1993;34:116-9. Crossref
3. Klinich KD, Schneider LW, Moore JL, Pearlman MD.
Injuries to pregnant occupants in automotive crashes.
Annu Proc Assoc Adv Automot Med 1998;42:57-91.
4. Bunai Y, Nagai A, Nakamura I, Ohya I. Fetal death from
abruptio placentae associated with incorrect use of a
seatbelt. Am J Forensic Med Pathol 2000;21:207-9. Crossref
5. Jamjute P, Eedarapalli P, Jain S. Awareness of correct use of a
seatbelt among pregnant women and health professionals:
a multicentric survey. J Obstet Gynaecol 2005;25:550-3. Crossref
6. Johnson HC, Pring DW. Car seatbelts in pregnancy: the
practice and knowledge of pregnant women remain causes
for concern. BJOG 2000;107:644-7. Crossref
7. Ichikawa M, Nakahara S, Okubo T, Wakai S. Car seatbelt
use during pregnancy in Japan: determinants and policy
implications. Inj Prev 2003;9:169-72. Crossref
8. Taylor AJ, McGwin G Jr, Sharp CE, et al. Seatbelt use
during pregnancy: a comparison of women in two prenatal
care settings. Matern Child Health J 2005;9:173-9. Crossref
9. Weiss H, Sirin H, Levine JA, Sauber E. International survey
of seat belt use exemptions. Inj Prev 2006;12:258-61. Crossref
10. Transport Department, The Government of the Hong Kong
Special Administrative Region. Protect your unborn child
in a car. Available from: http://www.td.gov.hk/filemanager/en/content_174/belt-e.pdf. Accessed Aug 2016.
11. Yu CH, Chan LW, Lam WC, To WK. Pregnant women’s knowledge and consumption of long-chain omega-3 polyunsaturated fatty acid supplements. Hong Kong J Gynaecol Obstet Midwifery 2014;14:57-63.
12. Liang KY, Zeger SL. Longitudinal data analysis using
generalized linear models. Biometrika 1986;73:13-22. Crossref
13. Robertson LS. The validity of self-reported behavioral risk factors: seatbelt and alcohol use. J Trauma 1992;32:58-9.Crossref
14. Luley T, Fitzpatrick CB, Grotegut CA, Hocker MB, Myers
ER, Brown HL. Perinatal implications of motor vehicle
accident trauma during pregnancy: identifying populations
at risk. Am J Obstet Gynecol 2013;208:466.e1-5. Crossref
15. Grossman NB. Blunt trauma in pregnancy. Am Fam
Physician 2004;70:1303-10.
16. Chapter 13: Fortuitous deaths. Why mothers die: report on
confidential enquiries into maternal deaths in the United
Kingdom 1994-1996. London: Royal College of Obstetrics
and Gynaecologists Press; 2001.
17. Cantwell R, Clutton-Brock T, Cooper G, et al. Saving
Mothers’ Lives: Reviewing maternal deaths to make
motherhood safer: 2006-2008. The Eighth Report of the
Confidential Enquiries into Maternal Deaths in the United
Kingdom. BJOG 2011;118 Suppl 1:1-203. Crossref
18. Transport Department, The Government of the Hong
Kong Special Administrative Region. Be Smart, buckle
up. Available from: http://www.td.gov.hk/filemanager/en/content_174/seatbelt_leaflet.pdf. Accessed Aug 2016.
19. Transport Department, The Government of the Hong
Kong Special Administrative Region. Road Traffic Accident
Statistics Year 2013. Available from: http://www.td.gov.hk/en/road_safety/road_traffic_accident_statistics/2013/index.html. Accessed Aug 2016.
20. Transport Department, The Government of the Hong
Kong Special Administrative Region. Seat belt: safe
motoring guides. Available from: http://www.td.gov.hk/en/road_safety/safe_motoring_guides/seat_belt/index.html.
Accessed Aug 2016.
21. Transport Department, The Government of the Hong
Kong Special Administrative Region. Road Safety Bulletin;
March 2001. Available from: http://www.td.gov.hk/filemanager/en/content_182/rs_bulletin_04.pdf. Accessed
Aug 2016.
22. Wallace C. General practitioners knowledge of and
attitudes to the use of seat belts in pregnancy. Ir Med J
1997;90:63-4.