DOI: 10.12809/hkmj144287
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
CASE REPORT
Aplasia of the optic nerve
Daniel CW Tang, MB, BS, FRCR; Eric MW Man, FRCR, FHKAM (Radiology); Sunny CS Cheng, FRCR, FHKAM (Radiology)
Department of Radiology, Pamela Youde Nethersole Eastern Hospital, Chai Wan, Hong Kong
Corresponding author: Dr Daniel CW Tang (tcw717@ha.org.hk)
 Full
paper in PDF
Full
paper in PDF
Abstract
Aplasia of the optic nerve is an extraordinarily
rare congenital anomaly that affects one or both
optic nerves and is associated with the absence of
the central retinal vessel and retinal ganglion cells.
We report a case of unilateral optic nerve aplasia
in a 4-month-old infant who was found to have
left microphthalmos on routine postnatal checkup.
Family history, antenatal history, and systemic
evaluation were unremarkable. Magnetic resonance
imaging showed absent left optic nerve with left
microphthalmos. The optic chiasm was present
and slightly deviated towards the right side. The remaining cerebral and ocular structures were
normal.
Introduction
Optic nerve aplasia is a very rare congenital anomaly
that is typically unilateral, and is characterised by
congenital absence of the optic nerve, central retinal
vessels, and retinal ganglion cells.1 Bilateral cases
are exceedingly rare. Various ocular anomalies are
associated with it.
Case report
A female infant weighing 3225 g was born to a
26-year-old G1P1 female at full term via caesarean
section because the umbilical cord was around the
neck. She was found to have left microphthalmos
on routine postnatal check-up in December 2013 in
Hong Kong, at the age of 3 months. Family history
was negative for ocular or other birth defects. Her
mother was a housewife, with no history of any
major illness during the pregnancy and antenatal
workup was unremarkable. Physical examination
was unremarkable with normal development for her
age.
Eye examination of the infant at 4 months
revealed left microphthalmos, and a left convergent
squint with no definite visual following. The left pupil
did not react to light stimulation and a persistent
pupillary membrane was evident. Coloboma of the
left optic disc was suspected. Fundus examination
showed whitish choroidal atrophy with a flat optic
disc on the left side. Right eye examination including
fundus examination was unremarkable as were all
blood tests and urinalysis.
Magnetic resonance imaging performed at
4 months revealed left microphthalmos, with no
recognisable left optic nerve. The right optic nerve
was present and normal in size. The optic chiasm
was seen and slightly deviated towards the right side,
likely related to the absence of the left optic nerve
(Fig 1). Bilateral optic tracts and optic radiations
were symmetrical. The septum pellucidum and
corpus callosum were intact and all other cerebral
and ocular structures were unremarkable (Fig 2).
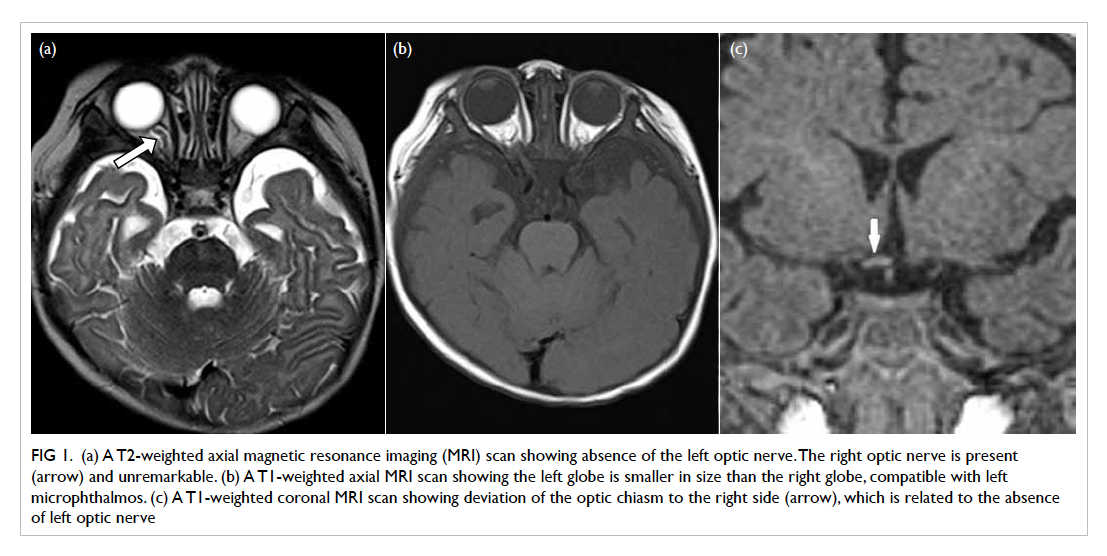
Figure 1. (a) A T2-weighted axial magnetic resonance imaging (MRI) scan showing absence of the left optic nerve. The right optic nerve is present (arrow) and unremarkable. (b) A T1-weighted axial MRI scan showing the left globe is smaller in size than the right globe, compatible with left microphthalmos. (c) A T1-weighted coronal MRI scan showing deviation of the optic chiasm to the right side (arrow), which is related to the absence of left optic nerve
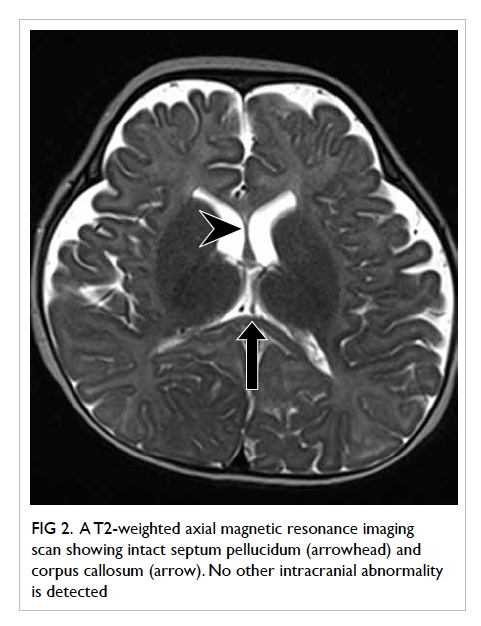
Figure 2. A T2-weighted axial magnetic resonance imaging scan showing intact septum pellucidum (arrowhead) and corpus callosum (arrow). No other intracranial abnormality is detected
Discussion
Aplasia of the optic nerve is a rare congenital anomaly
that is typically unilateral. It occurs sporadically in
an otherwise healthy person without sexual or racial
predilection,2 or any evidence of an inherited factor.
Prenatal history is usually normal, but the
possible influence of external factors such as
episodes of viral infection in the first trimester,3
acetone exposure, or smoking during pregnancy4
cannot be excluded.
The pathogenesis of optic nerve aplasia
remains unclear although it was first described 140
years ago. Scheie and Adler5 suggested that the defect
in aplasia was failure of the mesoderm to enter the
fetal fissure and provide vascularisation of the retina
and nerve tissue. Weiter et al6 doubted the defective
mesodermal development, since the dural sheath (a
mesodermal derivative) was present in the majority
of their cases. Instead, they suggested that the
ventral invagination of the optic vesicle causes nerve
fibre misdirection and secondary atrophy. Yanoff et
al7 postulated a primary failure of the ganglion cell
to develop and send out axons, resulting in a lack of
induction of mesodermal ingrowth including a lack
of retinal blood vessel development. Hotchkiss and
Green8 agreed that failure of mesodermal induction
was secondary to third-order neuronal defect in the
ganglion cell layer.
Plain X-ray can demonstrate a small optic
foramen on the side of aplasia.9 Computed
tomographic scan may show the globe and orbit on
the affected side to be smaller than the normal side.
Magnetic resonance imaging will show the absence
of optic nerve on the affected side. The chiasm and
lateral geniculate body may also appear small.10
Histopathological findings in optic nerve
aplasia include the absence of ganglion cells and
their axons as well as the absence of retinal vessels.7
According to many previous statements,
aplasia of the optic nerve is a part of hypoplasia
of the optic spectrum. According to an analysis
performed by Alqahtani,2 of 42 cases in the literature,
29 were genuine aplasia of the optic nerve, while the remainder were hypoplastic optic nerve.
Unilateral aplasia of the optic nerve is often
present in malformed eyes, with no abnormality
in brain tissue. Possible malformations of the eye
include microphthalmos, cataract, retinal dysplasia,
coloboma of the iris and ciliary body, iris hypoplasia,
malformation of the chamber angle, and persistent
hyperplastic primary vitreous.11 No light perception
is present in the affected eye and light stimulation
elicits no direct or consensual pupillary response.
Light stimulation of the normal eye results in a
direct or consensual pupillary response.11 Possible
malformation of the central nervous system includes
hydranencephaly, orbital meningoencephalocele,
and anencephaly.5 6
The prognosis of optic nerve aplasia is poor.
There is no specific treatment and blindness occurs
in the affected eye. Management of such cases
is directed towards identifying any associated
ophthalmological or neurological problems.
Cavallini et al12 recommended ocular prosthesis
in patients with associated microphthalmos, to
enable normal development of the orbit, at least for
aesthetic purposes.
Optic nerve aplasia should be suspected in a
patient who presents with unilateral microphthalmos
that is associated with the absence of central retinal
vessels and ganglion cells. Magnetic resonance
imaging is useful to screen for other associated
intracranial abnormality.
References
1. Blanco R, Salvador F, Galan A, Gil-Gibernau JJ. Aplasia of
the optic nerve: report of three cases. J Pediatr Ophthalmol Strabismus 1992;29:228-31.
2. Alqahtani J. Optic nerve aplasia: a case report and literature
review. J Pediatr Neurosci 2008;3:150-3. Crossref
3. Ginsberg J, Bove KE, Cuesta MG. Aplasia of the optic nerve
with aniridia. Ann Ophthalmol 1980;12:433-9.
4. Barry DR. Aplasia of the optic nerves. Int Ophthalmol
1985;7:235-42. Crossref
5. Scheie HG, Adler FH. Aplasia of the optic nerve. Arch
Ophthalmol 1941;26:61-70. Crossref
6. Weiter JJ, McLean IW, Zimmerman LE. Aplasia of the
optic nerve and disk. Am J Ophthalmol 1977;83:569-76. Crossref
7. Yanoff M, Rorke LB, Allman MI. Bilateral optic system
aplasia with relatively normal eyes. Arch Ophthalmol
1978;96:97-101. Crossref
8. Hotchkiss LH, Green WR. Optic nerve aplasia and
hypoplasia. J Pediatr Ophthalmol Strabismus 1979;16:225-40.
9. Little LE, Whitmore PV, Wells TW Jr. Aplasia of the optic
nerve. J Pediatr Ophthalmol 1976;13:84-8.
10. Margo CE, Hamed LM, Fang E, Dawson WW. Optic nerve
aplasia. Arch Ophthalmol 1992;110:1610-3. Crossref
11. Howard MA, Thompson JT, Howard RO. Aplasia of the
optic nerve. Trans Am Ophthalmol Soc 1993;91:267-76;
discussion 276-81.
12. Cavallini GM, Forlini M, Gramajo AL, et al. Optic nerve
aplasia and microphthalmos: a case report. J Genet Syndr
Gene Ther 2013;4:175. Crossref