Hong Kong Med J 2015 Jun;21(3):286.e2–3
DOI: 10.12809/hkmj144384
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Bisphosphonate-associated atypical femur fracture in a 90-year-old Caucasian woman
KG Gopinath, MD, FRACP; PK Shibu, FRACP, MRCP
Aged and Extended Care Services, The Queen Elizabeth Hospital, Woodville SA 5011, University of Adelaide, SA 5000, Australia
Corresponding author: Dr KG Gopinath (gops95@yahoo.com)
 Full
paper in PDF
Full
paper in PDF
A 90-year-old Caucasian female was admitted to the
hospital following a fall preceded by left thigh pain for
2 weeks in May 2013. Her medical history included
postmenopausal osteoporosis, depression, ischaemic
heart disease, and atrial fibrillation. She was on
alendronate for 11 years, as well as aspirin, bisoprolol,
digoxin, calcium, vitamin D, frusemide, metformin,
paracetamol, pantoprazole, and sertraline for around
14 years prior to hospital admission.
The Figure shows an atypical diaphyseal
fracture of the femur commonly associated with
long-term bisphosphonate therapy. These fractures
usually occur in patients taking bisphosphonates for
more than 5 years although it is known to occur with
shorter duration of usage and in bisphosphonate-naïve
patients (10%).1 This patient fulfilled all the
ASBMR (American Society for Bone and Mineral
Research) task force major and minor criteria for
atypical fractures.2 The mandatory major criterion
is fracture located along the femoral diaphysis from
just distal to the lesser trochanter to just proximal
to the supracondylar flare. In addition, at least
four of five major features must be present: (1) The
fracture is associated with minimal or no trauma,
as in a fall from a standing height or less. (2) The
fracture line originates at the lateral cortex and is
substantially transverse in its orientation, although
it may become oblique as it progresses medially
across the femur. (3) Complete fractures extend
through both cortices and may be associated with a
medial spike; incomplete fractures involve only the
lateral cortex. (4) The fracture is non-comminuted
or minimally comminuted. (5) There is localised
periosteal or endosteal thickening of the lateral
cortex at the fracture site (“beaking” or “flaring”). The
minor features not essential for diagnosis include:
generalised increase in cortical thickness of the
femoral diaphysis, unilateral or bilateral prodromal
symptoms such as dull or aching pain in the groin
or thigh, bilateral incomplete or complete femoral
diaphysis fracture, and delayed fracture healing.
Differential diagnoses in these patients include
femoral fractures with subtrochanteric extension,
pathological fractures associated with tumours, and
periprosthetic fractures.2
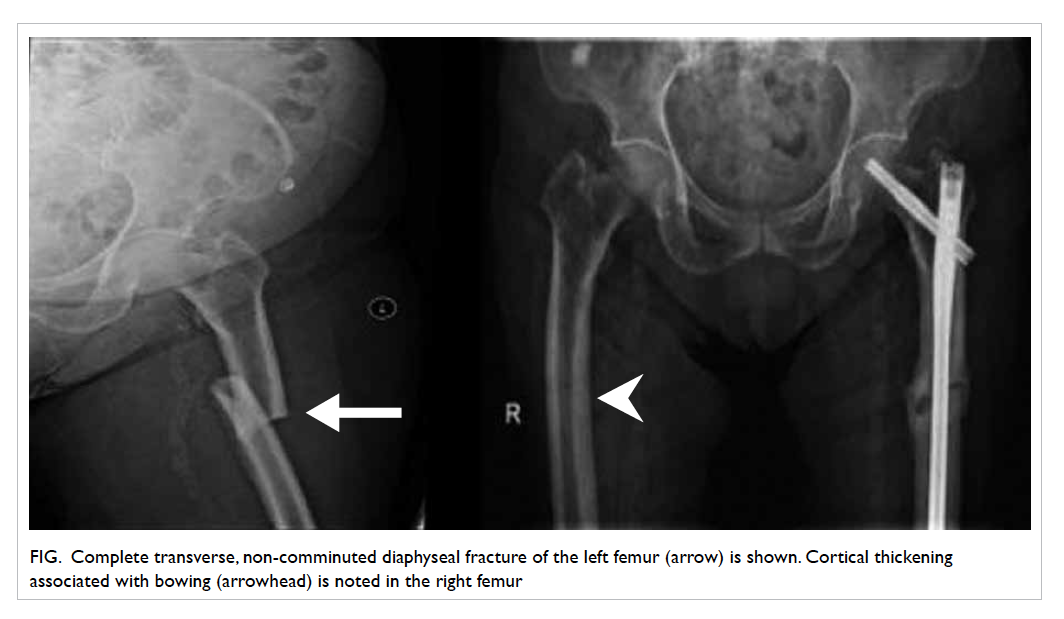
Figure. Complete transverse, non-comminuted diaphyseal fracture of the left femur (arrow) is shown. Cortical thickening associated with bowing (arrowhead) is noted in the right femur
Management strategies include cessation
of bisphosphonates, protected weight-bearing,
prophylactic intramedullary rod insertion, and
use of anabolic bone agents like teriparatide or
strontium.3 It is unclear whether a drug holiday is
useful to prevent these fractures.4 Our patient was
treated with intramedullary nailing and commenced
on strontium after cessation of bisphosphonates.
Greater awareness of this condition would prevent
misdiagnosis especially in frail older patients and
facilitate proper management.
Declaration
Dr PK Shibu has received educational grants
and honorarium from Novartis Pty Australia for
Osteoporosis and Fracture Liaison related clinical
research projects or lectures in the past and received
honorarium from Amgen Ltd for presenting at
educational meetings in the past.
References
1. Dell RM, Adams AL, Greene DF, et al. Incidence of
atypical nontraumatic diaphyseal fractures of the femur. J
Bone Miner Res 2012;27:2544-50. Crossref
2. Shane E, Burr D, Abrahamsen B, et al. Atypical
subtrochanteric and diaphyseal femoral fractures: second
report of a task force of the American Society for Bone
and Mineral Research. J Bone Miner Res 2014;29:1-23. Crossref
3. Carvalho NN, Voss LA, Almeida MO, Salgado CL,
Bandeira F. Atypical femoral fractures during prolonged
use of bisphosphonates: short-term responses to
strontium ranelate and teriparatide. J Clin Endocrinol
Metab 2011;96:2675-80. Crossref
4. Diab DL, Watts NB. Bisphosphonate drug holiday:
who, when and how long. Ther Adv Musculoskelet Dis 2013;5:107-11. Crossref