Hong Kong Med J 2015 Apr;21(2):131–5 | Epub 19 Dec 2014
DOI: 10.12809/hkmj134124
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Anterior cruciate ligament tear in Hong Kong Chinese patients
August WM Fok, FHKCOS, FHKAM (Orthopaedic Surgery); WP Yau, FHKCOS, FHKAM (Orthopaedic Surgery)
Division of Sports and Arthroscopic Surgery, Department of Orthopaedics
and Traumatology, Queen Mary Hospital, The University of Hong Kong, Hong Kong
Corresponding author: Dr August WM Fok (augustfok@hotmail.com)
 Full
paper in PDF
Full
paper in PDF
Abstract
Objective: To investigate the associations between
patient sex, age, cause of injury, and frequency of
meniscus and articular cartilage lesions seen at the
time of the anterior cruciate ligament reconstruction.
Design: Case series.
Setting: University affiliated hospital, Hong Kong.
Patients: Medical notes and operating records of 672
Chinese patients who had received anterior cruciate
ligament reconstruction between January 1997 and
December 2010 were reviewed. Data concerning all
knee cartilage and meniscus injuries documented at
the time of surgery were analysed.
Results: Of the 593 patients, meniscus injuries were
identified in 315 (53.1%). Patients older than 30
years were more likely to suffer from meniscal injury
compared with those younger than 30 years (60% vs
51%, P=0.043). Longer surgical delay was observed
in patients with meniscal lesions compared with
those without (median, 12.3 months vs 9.1 months, P=0.021).
Overall, 139 cartilage lesions were identified in 109
(18.4%) patients. Patients with cartilage lesions were
significantly older than those without the lesions
(mean, 27.6 years vs 25.1 years, P=0.034). Male
patients were more likely to have chondral injuries
than female patients (20.1% vs 10.9%, P=0.028). The
risk of cartilage lesions was increased by nearly 3
times in the presence of meniscal tear (P<0.0001;
odds ratio=2.7; 95% confidence interval, 1.7-4.2).
Conclusions: Increased age and surgical delay
increased the risk of meniscal tears in patients with
anterior cruciate ligament tear. Increased age, male
sex, and presence of meniscal tear were associated
with an increased frequency of articular lesions after
an anterior cruciate ligament tear.
New knowledge added by this
study
- This study served to identify the risk factors for meniscal and cartilage injuries in patients with anterior cruciate ligament (ACL) tear.
- Patients with ACL deficiency should be informed about the increased risk of meniscus injuries associated with surgical delay.
Introduction
Anterior cruciate ligament (ACL) tear is one of the
commonest sport injuries seen in clinical practice,
and such injury is often associated with meniscal
and chondral lesions. It is widely believed that early
surgery can prevent such lesions in ACL-deficient
patients, and probably help avoid the most dreadful
complication of early osteoarthritis of the knee.1
Despite multiple studies conducted to evaluate the
relationship between intra-articular injuries and
ACL tear, such associations among Asians, especially
Chinese, have not been extensively studied.
Data show that females are more susceptible
to ACL injury than their male counterparts,2 3 4 but
lower risk of other intra-articular injuries in females
was observed in some studies.5 Furthermore, a
study showed that the incidence of meniscus tear
was associated with the mechanism of ACL injury6;
however, other studies were not able to show a
significant relationship between the type of sports
causing injury and the incidence of meniscal and
chondral lesions.7
The objective of this study was two-fold. Our
first aim was to report the meniscal and chondral
lesions that accompany ACL tears in a large
Chinese population. Our second aim was to test for
relationships between the aforementioned lesions
and patient sex, age, surgical delay, and causes of
ACL injury.
Methods
A database that recorded all patients who had
received ACL reconstruction in our hospital since
1997 was reviewed. Overall, 672 Chinese patients
who had received the surgery between January 1997
and December 2010 were identified. Their medical
notes and operating records were reviewed. Data
concerning the patient sex, age, causes of injury,
elapsed time from injury to surgery, and all knee
cartilage and meniscus injuries documented at the
time of surgery were analysed.
Exclusion criteria were: patients who had
radiological evidence of osteoarthritis (Kellgren-Lawrence grade 3 or 4); a concomitant grade
III medial collateral ligament, lateral collateral
ligament, or posterior cruciate ligament deficiency
(evaluated and recorded by means of examination
with the patient under anaesthesia at the time of
surgery); any revision procedure involving the ACL;
or knee dislocation.
The time of the initial ACL injury was
determined from the patient’s history. This included
a definite incident of a single twisting injury, with
the knee giving away with a ‘pop’ sound, gross
knee swelling, and inability to resume the sport
or walking. The nature of this injury was further
verified with the hospital medical notes, or records
of the primary attending physician, when available.
Patients were considered potential candidates for
ACL reconstruction if any two of the following
criteria were satisfied: (1) instability during pivoting movements; (2) signs of ACL deficiency, including
a positive Lachman test, anterior drawer test, or a
positive pivot shift test; and (3) evidence of an ACL
tear on magnetic resonance imaging (MRI).
The presence of cartilage injuries and meniscal
lesions was confirmed in the operating room by
means of knee arthroscopy. Several independent
variables were studied: patient sex, age at the time
of surgery, surgical delay (defined as the duration
in months between the index ACL injury and
reconstruction), and causes of ACL injury.
Statistical analyses
Data analysis was performed using the Statistical
Package for the Social Sciences (Windows version
15.0; SPSS Inc, Chicago [IL], US). Student’s t test
was used to compare the means of the age. Mann-Whitney U test was used to compare the means of the
length of surgical delay. Fisher’s exact test was used
to evaluate the categorical variables. Binary logistic
regression was used to calculate the independent
effects of individual factors. A P value of <0.05 was
considered to be statistically significant.
Results
Of 672 patients who received ACL reconstruction,
79 were excluded (7 with concomitant high-grade
ligament deficiency, and 72 with revision ACL
surgery) and 593 patients were considered for
analysis. These included 483 (81%) males and 110
(19%) females. There were 297 (50%) right and 296
(50%) left knees. Their mean age at the time of surgery
was 26 years (range, 13-51 years), and their median
length of surgical delay was 10.5 months (range, 0.4-241.8 months).
Most of the patients had had their injuries
during sports activities (89.5%), with soccer (n=226,
42.6%) and basketball (n=163, 30.7%) being the
two most common sports (Tables 1 and 2). The age
distribution of patients having meniscal and cartilage
injuries is shown in Table 3. The incidence of intra-articular
lesions in different sports activities leading
to injury is shown in Table 4.
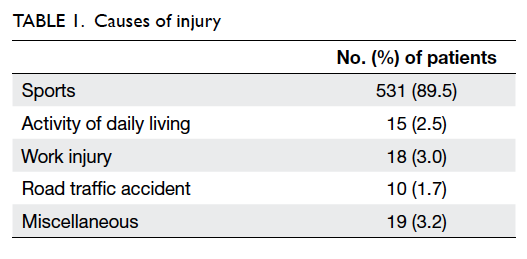
Table 1. Causes of injury
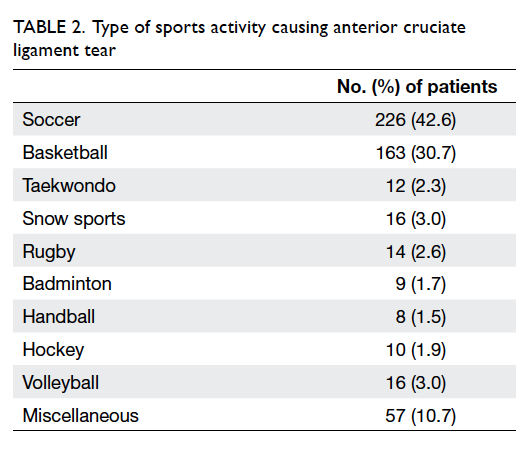
Table 2. Type of sports activity causing anterior cruciate ligament tear
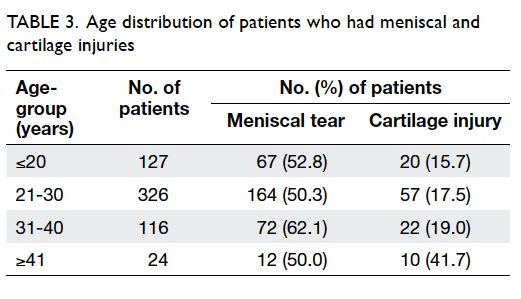
Table 3. Age distribution of patients who had meniscal and cartilage injuries
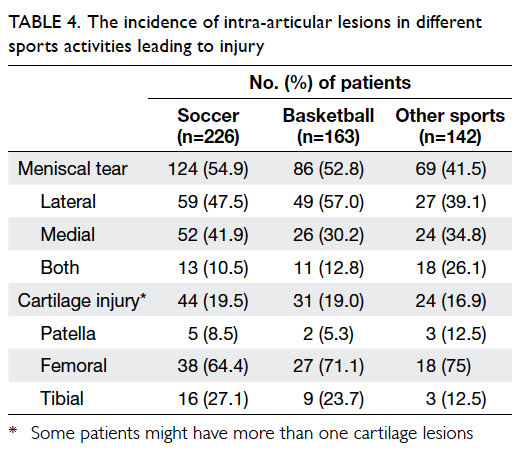
Table 4. The incidence of intra-articular lesions in different sports activities leading to injury
Meniscus injuries were identified in 315
(53.1%) patients. There were 146 (24.6%) isolated
lateral tears, 123 (20.7%) isolated medial tears, and
46 (7.8%) bilateral tears.
Patients older than 30 years were more likely
to suffer from meniscal injury versus those younger
than 30 years (60% vs 51%; P=0.043 by Fisher’s exact
test). Longer surgical delay was observed in patients
with meniscal lesions versus those without such
lesions (median, 12.3 months vs 9.1 months; P=0.021
by Mann-Whitney U test). Also, patients with medial
meniscal tear had a longer surgical delay than those
with lateral meniscal tear (median, 16.7 months
vs 9.0 months; P<0.001, Mann-Whitney U test). However, no significant associations were observed
between sex, causes of injury, type of sports, and
presence of meniscal lesions.
Overall, 139 cartilage lesions were identified in
109 (18.4%) patients. There were 16 patella (11.5%)
lesions, 92 (66.2%) femoral condyle lesions, and 31
(22.3%) tibial plateau lesions. Patients with cartilage
lesions were significantly older than those without
the lesions (mean, 27.6 years vs 25.1 years; P=0.034
by Student’s t test). Female patients were less likely
to suffer from chondral injuries than male patients
(10.9% vs 20.1%; P=0.028 by Fisher’s exact test).
Female sex was found to be independently associated
with incidence of cartilage injury in binary logistic
regression (P=0.029; odds ratio [OR]=0.475; 95%
confidence interval [CI], 0.243-0.929) [Table 5].
Presence of meniscal tear was associated with a
3-fold increased risk of cartilage lesions (P<0.001 by
Fisher’s exact test; OR=2.7, 95% CI, 1.7-4.2).

Table 5. Binary logistic regression for the factors associated with risk of cartilage injury
No significant association, however, was found
between surgical delay, causes of injury, type of
sports, and cartilage lesions.
Discussion
Our study showed that longer surgical delay was
present in patients with meniscal lesions, a finding
that concurs with data from other published
literature. Although Slauterbeck et al,5 Piasecki et
al,8 and O’Connor et al9 reported that female patients
had a lower rate of meniscus injury than male
patients, such association was not observed in our
study which recruited a lower proportion of female
patients; similar observation was made in the study
by Murrell et al.10
It is postulated that in acute ACL injury,
excessive anterolateral rotation of the tibia on
the femur traps the lateral meniscus between the
posterolateral aspect of the tibial plateau and the
central portion of the lateral femoral condyle. The
lateral meniscus is susceptible to a tear when the
tibia reduces. However, the scenario is different in
patients with chronic ACL deficiency. Recurrent
anterior translation of tibia on the femur results
in increased stress on the more stably fixed medial
meniscus due to the coronary ligaments, leading to a
subsequent medial meniscal tear.11 Our study found
that ACL-deficient patients with medial meniscus
tear had a mean of 9 months longer surgical delay
than those with lateral meniscus tear. Mitsou and
Vallianatos12 reported that the incidence of medial
meniscal tears increased from 17% in patients with
ACL reconstruction within 3 weeks of injury to
48% in those who had surgery of more than 6 months
after injury; such risk was not observed in lateral
meniscus tears. O’Connor et al9 found that patients
who underwent ACL reconstruction more than 2
years after injury had only 1.5 times increased risk in
lateral meniscus injuries, but 2.2 times increased risk
in medial meniscus injuries.
In our study, males were found to have higher
incidence of cartilage defect than females, but there
was no significant difference in terms of meniscal
lesions. Slauterbeck et al5 found that male sex was
associated with an increased risk of meniscal and
chondral lesions in ACL-deficient patients. In a study
by Piasecki et al,8 female high-school athletes were
found to have fewer meniscal tears (while playing
soccer) and a reduced number of intra-articular
injuries to the medial femoral condyle while playing
basketball, but such associations were not observed
among amateur athletes. So far, there has been little
research on sex differences in articular cartilage
injuries accompanying ACL tears. Granan et al13
reported that cartilage lesions were nearly twice as
frequent if there was a meniscal tear, and similar
observations were found in our study.
The association of age with meniscus tear and
cartilage injury with intact ACL is less extensively
studied. In a cross-sectional MRI study of nearly
1000 individuals from the general population who
were aged 50 to 90 years, 31% of knees were found
to have a meniscal tear and the incidence increased
with age. It was shown that 21% of the 50- to
59-year-old subjects had a meniscal tear, compared
to 46% of subjects aged 70 to 90 years.14 In several
large-scale retrospective studies which reviewed the
articular cartilage defects during knee arthroscopy,
the incidence of isolated chondral lesions without
associated intra- and extra-articular knee lesions
ranged from 30% to 36.6%.15 16 17 18 No significant
statistical associations, however, were found between
age and the cartilage lesions.
Studies have shown that individuals who
participate in vigorous physical activities are
more disabled by an ACL injury than those who
are relatively sedentary. Paul et al6 reported an
association between the mechanism of an ACL
injury (jumping and non-jumping) and the incidence
of concomitant meniscus injuries, but other authors
failed to show such associations. In our study, since more than
half of the patients were injured while playing soccer
or basketball, an analysis was performed to evaluate
if the soccer and basketball players suffered from
lesions that were different from those sustained
from other causes or during other sports activities.
However, type of sports was not associated with
any of the parameters we studied. A larger sample
including patients with other causes of injury will be
needed to prove if there are differences among other
sports activities.
Another limitation of this study was that
patients receiving conservative treatment for their
ACL injury were not recruited in the present study.
This could lead to potential bias as their risks of
meniscal and articular injuries could not be estimated.
We are also aware that more sophisticated systems
to evaluate the meniscal and chondral lesions, eg the
Cooper’s classification19 and the ICRS (International
Cartilage Repair Society) classification system,20
could be used to map the lesions, so as to provide
more precise anatomical description and details of
the lesions.
Compared with other studies, which report
surgical delay ranging from 1.2 to 13 months,5 6 7 9 10 11
patients in our series had a longer surgical delay. Patients may have postponed the waiting time
for surgery or imaging including MRI. It was unclear
if patients would suffer from repeated knee injuries,
or the activities in which the patients were involved before the surgery would have any effect over the
findings of our study.
Currently, there is intense debate concerning
the optimal timing for ACL reconstruction.21 22
Different surgeons have different personal preferences.
Some prefer early surgery while others are in favour
of an optimal period of rehabilitation before
considering surgery. Frobell et al23 concluded in his
randomised controlled trial that “In young, active adults
with acute ACL tears, a strategy of rehabilitation
plus early ACL reconstruction was not superior to
a strategy of rehabilitation plus optional delayed
ACL reconstruction.” According to Richmond et al,22
however, Frobell’s conclusion is flawed; they believe
that prompt operative intervention reduces long-term
osteoarthritis after knee ACL tear. No matter
what approach the surgeons prefer, our patients with
ACL tear should be well informed about the risks
and benefits of conservative management versus
surgical reconstruction, so they can make their best
decision with the best information on hand.
Conclusions
Increased age and surgical delay were associated
with meniscal tear in patients with ACL tear, and
longer surgical delay was observed in patients with
medial meniscal tear. Increased age, male sex, and
presence of meniscal tear were all associated with
chondral lesions after an ACL tear. Cause of injury
or type of sports activity leading to ACL injury was
not associated with intra-articular lesions.
References
1. Lohmander LS, Englund PM, Dahl LL, Roos EM. The
long-term consequence of anterior cruciate ligament
and meniscus injuries: osteoarthritis. Am J Sports Med
2007;35:1756-69. Crossref
2. Arendt E, Dick R. Knee injury patterns among men and
women in collegiate basketball and soccer. NCAA data and
review of literature. Am J Sports Med 1995;23:694-701. Crossref
3. Bjordal JM, Arnly F, Hannestad B, Strand T. Epidemiology
of anterior cruciate ligament injuries in soccer. Am J Sports
Med 1997;25:341-5. Crossref
4. Messina DF, Farney WC, DeLee JC. The incidence of injury
in Texas high school basketball. A prospective study among
male and female athletes. Am J Sports Med 1999;27:294-9.
5. Slauterbeck JR, Kousa P, Clifton BC, et al. Geographic
mapping of meniscus and cartilage lesions associated with
anterior cruciate ligament injuries. J Bone Joint Surg Am
2009;91:2094-103. Crossref
6. Paul JJ, Spindler KP, Andrish JT, Parker RD, Secic M,
Bergfeld JA. Jumping versus nonjumping anterior cruciate
ligament injuries: a comparison of pathology. Clin J Sport
Med 2003;13:1-5. Crossref
7. Tandogan RN, Taşer O, Kayaalp A, et al. Analysis of
meniscal and chondral lesions accompanying anterior
cruciate ligament tears: relationship with age, time from
injury, and level of sport. Knee Surg Sports Traumatol
Arthrosc 2004;12:262-70. Crossref
8. Piasecki DP, Spindler KP, Warren TA, Andrish JT, Parker
RD. Intraarticular injuries associated with anterior cruciate
ligament tear: findings at ligament reconstruction in high
school and recreational athletes. An analysis of sex-based
differences. Am J Sports Med 2003;31:601-5.
9. O’Connor DP, Laughlin MS, Woods GW. Factors related
to additional knee injuries after anterior cruciate ligament
injury. Arthroscopy 2005;21:431-8. Crossref
10. Murrell GA, Maddali S, Horovitz L, Oakley SP, Warren RF.
The effects of time course after anterior cruciate ligament
injury in correlation with meniscal and cartilage loss. Am J
Sports Med 2001;29:9-14.
11. Duncan JB, Hunter R, Purnell M, Freeman J. Meniscal
injuries associated with acute anterior cruciate ligament
tears in alpine skiers. Am J Sports Med 1995;23:170-2. Crossref
12. Mitsou A, Vallianatos P. Meniscal injuries associated with
rupture of the anterior cruciate ligament: a retrospective
study. Injury 1988;19:429-31. Crossref
13. Granan LP, Bahr R, Lie SA, Engebretsen L. Timing of
anterior cruciate ligament reconstructive surgery and
risk of cartilage lesions and meniscal tears: a cohort study
based on the Norwegian National Knee Ligament Registry.
Am J Sports Med 2009;37:955-61. Crossref
14. Englund M, Guermazi A, Gale D, et al. Incidental meniscal
findings on knee MRI in middle-aged and elderly persons.
N Engl J Med 2008;359:1108-15. Crossref
15. Arøen A, Løken S, Heir S, et al. Articular cartilage lesions
in 993 consecutive knee arthroscopies. Am J Sports Med
2004;32:211-5. Crossref
16. Curl WW, Krome J, Gordon ES, Rushing J, Smith BP,
Poehling GG. Cartilage injuries: a review of 31,516 knee
arthroscopies. Arthroscopy 1997;13:456-60. Crossref
17. Hjelle K, Solheim E, Strand T, Muri R, Brittberg M.
Articular cartilage defects in 1,000 knee arthroscopies.
Arthroscopy 2002;18:730-4. Crossref
18. Widuchowski W, Widuchowski J, Trzaska T. Articular
cartilage defects: study of 25,124 knee arthroscopies. Knee
2007;14:177-82. Crossref
19. Cooper DE, Arnoczky SP, Warren RF. Meniscal repair. Clin
Sports Med 1991;10:529-48.
20. Brittberg M, Winalski CS. Evaluation of cartilage injuries
and repair. J Bone Joint Surg Am 2003;85-A Suppl 2:58-69.
21. Bernstein J. Early versus delayed reconstruction of the
anterior cruciate ligament: a decision analysis approach. J
Bone Joint Surg Am 2011;93:e48. Crossref
22. Richmond JC, Lubowitz JH, Poehling GG. Prompt
operative intervention reduces long-term osteoarthritis
after knee anterior cruciate ligament tear. Arthroscopy
2011;27:149-52. Crossref
23. Frobell RB, Roos EM, Roos HP, Ranstam J, Lohmander LS.
A randomized trial of treatment for acute anterior cruciate
ligament tears. N Engl J Med 2010;363:331-42. Crossref