Hong Kong Med J 2014 Aug;20(4):297–303 | Epub 23 May 2014
DOI: 10.12809/hkmj134074
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Factors associated with intimate partner
violence against women in a mega city of South-Asia: multi-centre
cross-sectional study
Niloufer S Ali, MB, BS, FCPS1;
Farzana N Ali, MB, BS2; Ali K Khuwaja, MB, BS, FCPS3;
Kashmira Nanji, MSc, BScN1
1 Department of Family
Medicine, The Aga Khan University, Karachi
74800, Pakistan
2 Department of Family
Medicine and Community Health, University
Hospitals Case Medical Center, Ohio 44106, United States
3 Departments of Family
Medicine/Community Health Sciences, The Aga
Khan University, Karachi 74800, Pakistan
Corresponding author: Dr Kashmira Nanji (kashmira.nanji@aku.edu)
 Full
paper in PDF
Full
paper in PDF
Abstract
Objectives: To assess
the proportion of women
subjected to intimate partner violence and the
associated factors, and to identify the attitudes
of women towards the use of violence by their
husbands.
Design: Cross-sectional
study.
Setting: Family practice
clinics at a teaching hospital
in Karachi, Pakistan.
Participants: A total of
520 women aged between
16 and 60 years were consecutively approached
to participate in the study and interviewed by
trained data collectors. Overall, 401 completed
questionnaires were available for analysis.
Multivariate logistic regression analysis was used to
identify the association of various factors of interest.
Results: In all, 35% of
the women reported being
physically abused by their husbands in the last
12 months. Multivariate analysis showed that
experiences of violence were independently
associated with women’s illiteracy (adjusted odds
ratio=5.9; 95% confidence interval, 1.8-19.6),
husband’s illiteracy (3.9; 1.4-10.7), smoking habit of husbands
(3.3; 1.9-5.8), and substance use (3.1; 1.7-5.7).
Conclusion: It is
imperative that intimate partner
violence be considered a major public health
concern. It can be prevented through comprehensive,
multifaceted, and integrated approaches. The role
of education is greatly emphasised in changing the
perspectives of individuals and societies against
intimate partner violence.
New knowledge added by this
study
- This study shows that women’s literacy can play an important role in changing the perspectives of individuals and societies towards violence against women.
- Substance abuse including smoking and alcohol consumption may directly be responsible for intimate partner violence against women in Pakistan.
- The growing understanding of the impact of violence needs to be translated into primary, secondary, and tertiary level prevention, including both services that respond to the needs of women living with or who have experienced violence, and interventions to prevent violence.
- There is a need for intervention programmes in all societies and cultures for both men and women to highlight this imperative issue.
Introduction
Intimate partner violence (IPV) against
women is
a global human rights and public health problem.
Addressing violence against women (VAW) is central
to the achievement of Millennium Development
Goal (MDG) 3 on women’s empowerment and
gender equality, as well as MDGs 4, 5, and 6.1 Intimate
partner violence is defined as “the range of sexually,
psychologically and physically coercive acts used
against adult and adolescent women by current or
former male intimate partners”.2
The two terms, VAW and IPV, are used
interchangeably with gender-based violence. It
is reported that violence imposed by husbands is
the most common form of VAW.3
Data from the
World Bank suggest that women aged 15 to 44
years are at greater risk from rape and domestic
violence than from cancer, motor accidents, war,
and malaria.3 There is
enormous body of evidence
to suggest that such acts of violence adversely affect
the overall wellbeing of women and are associated
with psychiatric morbidities like anxiety, depression, addictive
behaviour, etc, and physical injuries,
sexually transmitted infections, poor reproductive
health outcomes, and even death.4
5 6 7 The
impact may
also span to affect the mental and physical health of
children, who may get “caught in the cross fire” and
are directly injured or may get less directly affected
as a consequence of abusive relationship between
parents.8 9
Violence against intimate partners occurs
in all
countries, all cultures, and at every level of society
without exception, although some populations (for
example, low-income groups) are at greater risk of
violence by intimate partners than others.10 In 48
population-based surveys from around the world,
10% to 69% of women reported being physically
assaulted by an intimate male partner at some point
in their lives.3 The World
Health Organization
(WHO) multi-country study on women’s health and
domestic violence documented lifetime prevalence
of physical and/or sexual partner violence among
ever-partnered women in the 15 sites surveyed
ranging from as low as 15% in an Ethiopian province
to as high as 71% in Japan.11
The burden of IPV is particularly alarming
in
developing countries as women are vulnerable to
many forms of violence and IPV represents the most
common form.
The widespread nature of the issue is
further evidenced by the findings of more recent
studies from countries with varied economic
and developmental strata. About 15% of women
visiting the family practitioners in Toronto, Canada, admitted
being victims of IPV.12
Another study
from a developing country reported the prevalence
of male partner–perpetrated violence to be around
7%.13 Although a true
comparison is difficult to
make due to methodological differences between
studies, in general, a higher burden of the problem
is observed in developing countries, including those
from South Asia. Around one third to one half of the
female participants in different studies from India
accept IPV victimisation.13
14 According to the recent
Bangladesh Demographic Health Survey, almost
half of married Bangladeshi mothers (42.4%) with
children aged 5 years and younger experienced IPV
from their husbands.14
Similarly, in Pakistan, nearly
one third to one half of the women stated that they
are victims of IPV.15 16
Although the prevalence of IPV varies
across
countries, the factors associated with an increased
risk of IPV are similar. These may include substance/alcohol use, young age, and attitudes supportive of
wife beating. However, higher education status, high
socio-economic status, and formal marriage offer
protection against IPV.11
17 18
Limited data are available from Pakistan on
VAW. The topic remains largely inadequately studied
despite its far-reaching adverse consequences.
Moreover, most of the published studies have
been conducted in the same communities or
in communities with similar socio-economic
backgrounds, skewing the approximate magnitude
of the problem to extremes and hampering the
analysis of important demographic factors that may
be associated with IPV against women. The aim of
this study was therefore to estimate the proportion of
women subjected to IPV in Pakistan and to examine
whether demographic factors such as education
status of both wife and husband and husband’s
involvement in substance abuse were associated
with IPV. We conducted this study among women
from diverse socio-economic backgrounds to assess
the proportion of women subjected to IPV and the
associated factors. We also aimed to determine the
attitudes of participants towards the use of violence
by husbands.
Methods
This cross-sectional study was conducted in
four
family practice clinics situated in various localities
of Karachi, the largest city and economic hub of
Pakistan. Karachi is one of the largest metropolitan
cities of the world where over 16 million people
reside; it is also called mini-Pakistan as its residents
represent all the ethnicities, provinces/states, and
socio-economic classes. All these clinics are affiliated
with a private tertiary care teaching hospital. A total
of eight family practice clinics are associated with the
teaching hospital and these clinics were included as
they provide health services to people from different
socio-economic strata (lower, middle, and upper). All
participants were assured of complete confidentiality
of the information collected. After obtaining consent
to participate in the study, currently married women
(aged 16-60 years) were interviewed consecutively
by four female medical students (each in a clinic)
who had received prior training for this task. The
data were collected simultaneously in all the clinics
from July 2012 to November 2012. Sample size was
calculated with the help of WHO software for sample
size determination. As the prevalence of VAW ranges
between 30% and 50%,14 15 16 we used a prevalence of
50% for maximum variance with an error bound of
5%; this gave a sample size of 385. The sample size
was then inflated by 7% for non-respondents to give
a final sample size of approximately 412.
After extensive literature search and
consensus
by study investigators, a structured questionnaire
was developed and pre-tested. The questionnaire
was initially prepared in English, translated into
Urdu and then back-translated into English. The final
questionnaire was comprised of sections including
socio-demographic characteristics and questions
regarding the experience of physical/verbal abuse
inflicted ever (lifetime) by husband. In this study,
physical abuse was defined by any of the following
acts used against women: slapping or throwing
something at her that could hurt her; pushing or
shoving; hitting with fist or something else that
could hurt; kicking, dragging, or beating; choking
or burning on purpose; and threatening to use or
actually use a gun, knife, or weapon against her. The
questionnaire also included a section on the women’s
attitude towards use of violence by husbands against
wives. Questions were also included about other
variables of interest which included education
status of the woman and her husband, working
status of the woman and her husband, years since
marriage and total number of children, family
system in which the woman lives, and information
about smoking status and other addictive substances
used by the husband. The time required to complete
the questionnaire was about 25 to 30 minutes. Due
to the sensitivity of the issue, the interviews were
conducted with each participant in separate rooms
ensuring full privacy. The study was approved by the
Research Committee of the Department of Family
Medicine, Aga Khan University, Karachi, Pakistan,
and prior permission was sought by administration
of study clinics.
Data were analysed using the Statistical Package for the
Social
Sciences (Windows version 19; SPSS Inc, Chicago
[IL], US). The proportion of violence experienced
by women and other variables of interest were
calculated. Cross-tabulation and Chi squared test
were used to assess the association between the women’s perception
and their level of education.
The independent association of factors studied with
violence experienced by women was examined by
multivariate stepwise logistic regression analysis
to obtain odds ratios (ORs) and 95% confidence
intervals (CIs). Covariates such as education status
of participants, education status of husband, and
smoking and substance abuse by husband were
included in the multivariate model.
Results
A total of 550 women were approached, of
which 520
fulfilled the eligibility criteria. As there were 119 women who refused to participate or provided incomplete information in the questionnaire, the response rate was
77%. Finally, information from 401 participants
was included in the final analysis; for missing data,
we averaged estimates of the variables to give a
single mean estimate. The socio-demographic
characteristics of the participants are summarised in
Table 1. Overall, 190 (47.4%) of the
participants were
aged 40 years and above, 165 (41.1%) had received
no education at all, and husbands of 111 (27.7%)
participants had received no schooling. A majority
(n=363; 90.5%) of respondents were housewives
while one third of the participants’ husbands were
not working (jobless or retired from work). Overall,
170 (42.4%) participants had been married for more
than 20 years, 265 (66.1%) had three or more children,
and 252 (62.8%) were living in nuclear (single)
families. Husbands of 132 (32.9%) participants were
current tobacco smokers and over one fifth of them
consumed addictive substances other than tobacco
smoking.
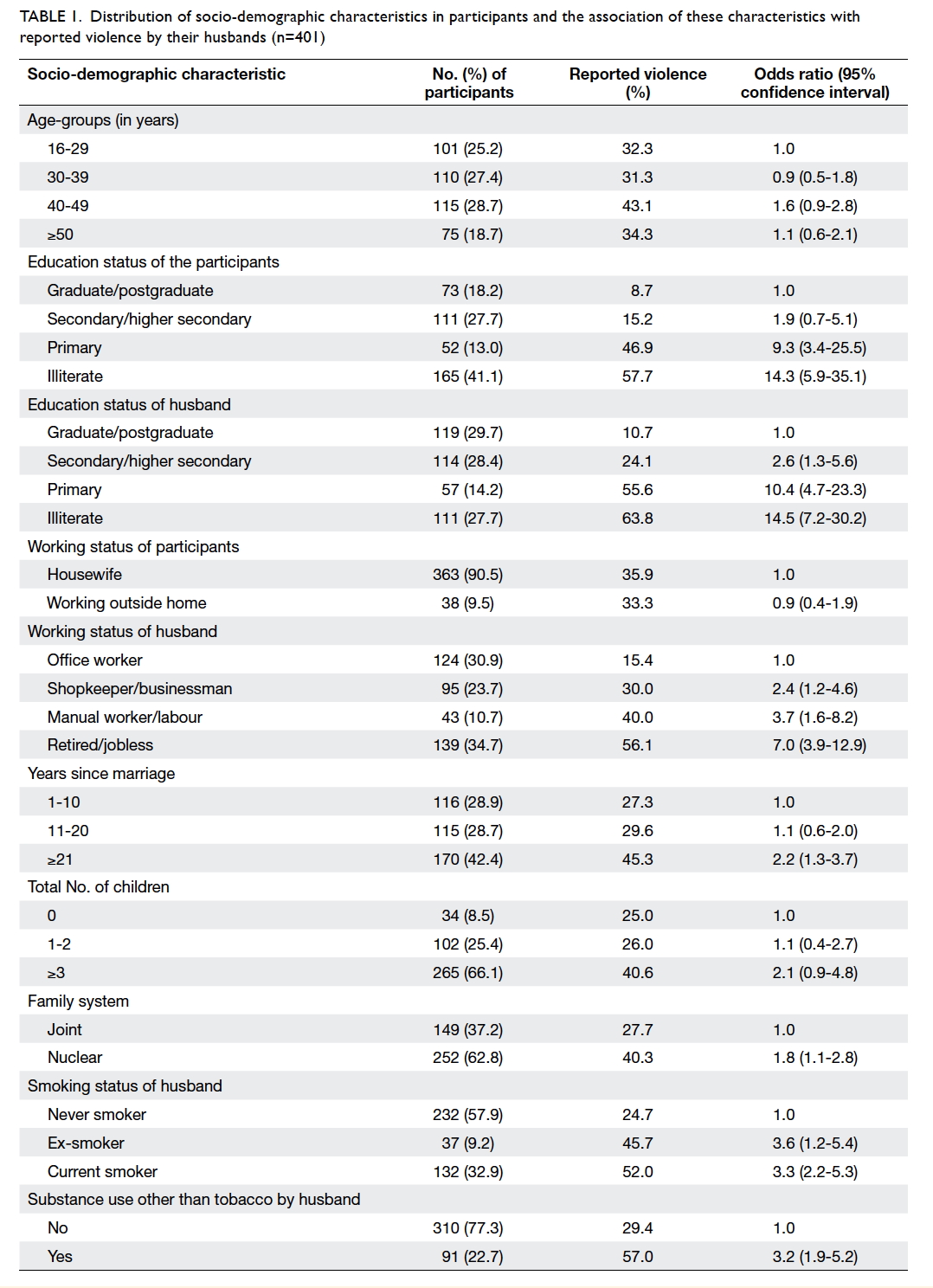
Table 1. Distribution of socio-demographic characteristics in participants and the association of these characteristics with reported violence by their husbands (n=401)
Overall, 140 (35%) participants reported
being ever physically/verbally violated by their
husbands in the last 12 months. The factors associated with IPV against
women on univariate analysis are summarised in
Table 1. These included illiteracy of women, living
in a nuclear family, and being married for more
than 20 years; factors related to the husband were
illiteracy, unemployment, smoking, and use of other
substances besides tobacco.
In the multivariate analysis (Table
2), four
factors were independently associated with IPV
against women. These were women’s illiteracy,
husband’s illiteracy, smoking habit of husband, and
use of substances other than tobacco by husband.
Women who were illiterate were 6 times more likely
to have been violated by their husbands versus
those who were literate (adjusted OR [AOR]=5.9;
95% CI, 1.8-19.6), while women whose husbands
were illiterate were 4 times more likely to have been
abused than those whose husbands were literate
(AOR=3.9; 95% CI, 1.4-10.7). Study participants
whose husbands smoked tobacco reported being
victims of violence by their husbands 3 times more
often than their counterparts (AOR=3.3; 95% CI,
1.9-5.8). Almost similar odds for IPV were observed in
participants whose husbands were addicted to
substances other than tobacco (AOR=3.1; 95% CI;
1.7-5.7).
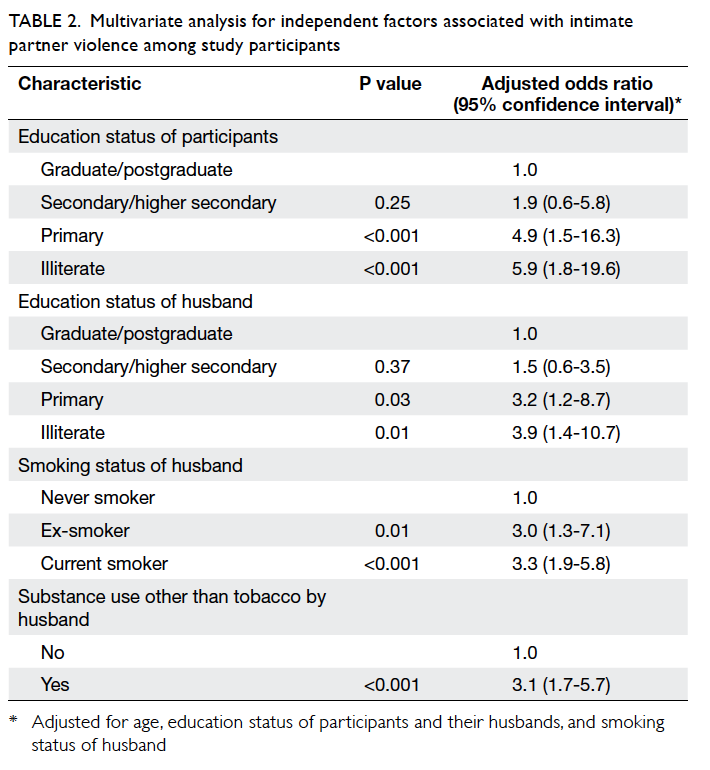
Table 2. Multivariate analysis for independent factors associated with intimate partner violence among study participants
Overall, 268 (67%) participants accepted
that a
wife should always follow her husband’s instructions
irrespective of her will and 74 (18.5%) women
agreed that violence against wife was justified if she
did not follow her husband’s instructions.
The association of women’s perspective
towards husband’s dominance and use of violence
against wife with the number of years of school
attended by women is shown in the Figure. As the
number of years of schooling increased, there was
a significant decline in the proportion of women
who were in favour of husbands’ dominance over
wives, and those who accepted violence against
wives (Chi squared, P<0.001). The Figure depicts
that the majority of the illiterate women (over 75%)
agreed that wife should always follow her husband’s
instructions irrespective of her will, and about 30%
believed that violence against a wife was justified if
she did not follow her husband’s instructions. On
the other hand, less than 5% of the women who had
more than 12 years of education thought that IPV
was justified if the husband’s instructions were not
followed.
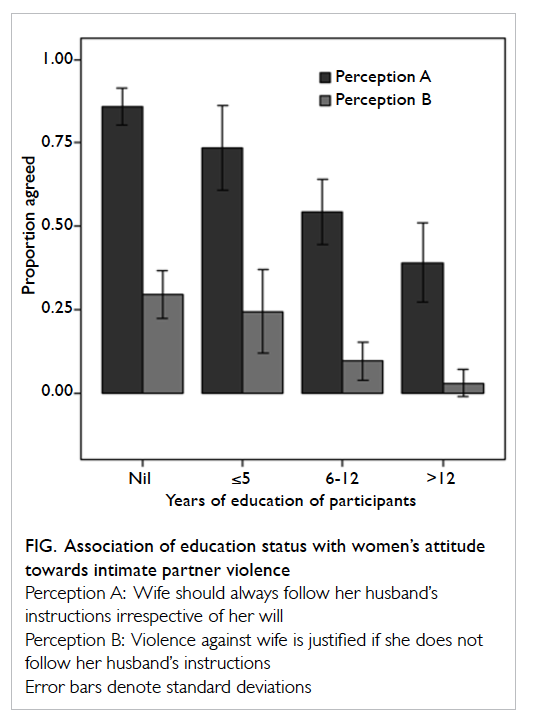
Figure. Association of education status with women’s attitude towards intimate partner violence
Discussion
Violence against women is being
increasingly
identified as a major contributor to the ill health and
mortality among women.3 10 Despite the imperative
nature of the problem, there is lack of adequate
information on IPV against women in Pakistan. In
the current study, we have explored the proportion
of women abused by their intimate partners and
have identified factors significantly associated with
such acts of abuse.
In this study, approximately one third of
the women (35%) reported being ever physically/verbally violated by their husbands. Other studies
from Pakistan15
16 have also reported similar findings,
with approximately one third to one half of the
participants experiencing some form of violence
from intimate partners. However, a study
conducted in Karachi, Pakistan, among 400 married
women showed that the prevalence of IPV (physical
violence) was 80%.17 A
possible explanation for this
high magnitude of IPV prevalence could be the fact
that the participants were recruited from low socio-demographic
background communities that may be
associated with increased perpetuation of violence
and vulnerability to the victimisation of violence.
The education status of both the partners
has been observed to have significant influence on
the prevalence of IPV.19 20 21 Provision of education
undoubtedly plays a protective role against IPV.
Empowering women through social networking
along with income earning improves their capacity to access
information and resources available in
society, and seek help in case of spousal abuse.19
The results of the current study also clearly indicate
a positive association between the literacy levels
of husband and wife and IPV victimisation among
women. Education also imparts a protective role
through influencing the perspectives of individuals,
and societies in general, against the acceptability
of mistreatment towards women.19
A climate
of tolerance towards IPV makes it easier for
perpetrators to persist with their violent behaviour.22
Education inculcates a sense of self-respect and self-reliance
in women, enhancing their capacity to make
appropriate decisions regarding various aspects
of their lives confidently and autonomously.11
On the other hand, lack of education not only
deprives women from acknowledging their rights
but, instead, stigmatises their thinking on gender
roles and makes them more accepting towards use
of force to impose these roles.23
24 This effect was
observed in previous studies in which low level of
education was associated with women’s acceptance
of wife battering, whereas higher education level
was negatively associated with tolerance of wife
beating. Furthermore, educated women were most
protected against violence.23
24 This is also reflected
in the findings of this study in that acceptance
and tolerance towards husband’s mistreatment
and control over the wife markedly declined as the
education level of the women improved.
The results of the current study also
indicate
that women whose husbands smoke or consume
other substances of abuse experience increased
levels of IPV. This is consistent with the findings
of previous studies20 25 26 which showed that smoking,
alcohol consumption, and using other substances
of abuse were strongly associated with IPV. Substance abuse, including smoking and alcohol
consumption, may be directly responsible for
IPV by affecting cognition, reducing self-control,
perpetuating aggression and may also induce stress
and unhappiness in relationships, thereby, further
increasing the risk of violence and conflict.26
This study has some limitations. It was
conducted in selective family practice clinics which
may have underestimated the results due to under-reporting.
Since these clinics are situated in urban
areas of a single city, the participants may not
represent the population at large. Moreover, the
response rate was low in this study (77%) due to the
sensitive nature of the issue. There is also a chance
of selection bias. As this was a cross-sectional study,
temporality or causality could not be established.
Owing to the cultural and social restrictions, we did
not enquire about sexual abuse. Moreover, due to
sensitivity of the issue, there may have been under-reporting
of such information. We had asked about
the abuse ever in the lifetime; therefore, there is some
possibility of recall bias as well. Hence, the actual
burden of the problem may be higher than what we
have reported. Finally, the questionnaire used in this
study is not a validated tool, so there is a chance of
information bias in the study.
Conclusion
In the light of the above findings, it is
imperative
that VAW be considered a major public health
concern. The prevention of VAW can be achieved
through comprehensive, multifaceted, and
integrated approaches that require joint efforts by
the government, policy-makers, social workers,
religious scholars, educationalists, and public health
practitioners. In this respect, the role of education
is greatly emphasised in changing the perspectives
of individuals and societies against IPV. Family
physicians, being the first-line doctors and health
care providers, should be well trained in screening
for IPV and providing instantaneous care to the
victims by catering to their psychological needs to prevent poor
mental health outcomes.
References
1. Hogan MC, Foreman KJ, Naghavi M,
et al. Maternal mortality for 181 countries, 1980-2008: a
systematic analysis of progress towards Millennium Development
Goal 5. Lancet 2010;375:1609-23. CrossRef
2. Heise L. Violence against women:
the hidden health burden. World Health Stat Q 1993;46:78-85.
3. Carolissen R. World report on
violence and health. S Afr Med J 2003;93:272.
4. Sarkar NN. The impact of
intimate partner violence on women’s reproductive health and
pregnancy outcome. J Obstet Gynecol 2008;28:266-71. CrossRef
5. Bailey BA, Daugherty RA.
Intimate partner violence during pregnancy: incidence and
associated health behaviors in a rural population. Matern Child
Health J 2007;11:495-503. CrossRef
6. Ruiz-Pérez I, Plazaola-Castaño
J, Del Río-Lozano M. Physical health consequences of intimate
partner violence in Spanish women. Eur J Public Health
2007;17:437-43. CrossRef
7. Abrahams N, Jewkes R, Martin LJ,
Mathews S, Vetten L, Lombard C. Mortality of women from intimate
partner violence in South Africa: a national epidemiological
study. Violence Vict 2009;24:546-56. CrossRef
8. Bair-Merritt MH, Blackstone M,
Feudtner C. Physical health outcomes of childhood exposure to
intimate partner violence: a systematic review. Pediatrics
2006;117:e278-90. CrossRef
9. Graham-Bermann SA, Gruber G,
Howell KH, Girz L. Factors discriminating among profiles of
resilience and psychopathology in children exposed to intimate
partner violence (IPV). Child Abuse Negl 2009;33:648-60. CrossRef
10. Garcia-Moreno C, Jansen HA,
Ellsberg M, et al. Prevalence of intimate partner violence:
findings from the WHO multi-country study on women’s health and
domestic violence. Lancet 2006;368:1260-9. CrossRef
11. Abramsky T, Watts CH,
Garcia-Moreno C, et al. What factors are associated with recent
intimate partner violence? Findings from the WHO multi-country
study on women’s health and domestic violence. BMC Public Health
2011;11:109. CrossRef
12. Ahmad F, Hogg-Johnson S,
Stewart DE, Levinson W. Violence involving intimate partners:
prevalence in Canadian family practice. Can Fam Physician
2007;53:460-8.
13. Chandra PS, Satyanarayana VA,
Carey MP. Women reporting intimate partner violence in India:
associations with PTSD and depressive symptoms. Arch Womens Ment
Health 2009;12:203-9. CrossRef
14. Silverman JG, Decker MR, Gupta
J, Kapur N, Raj A, Naved RT. Maternal experiences of intimate
partner violence and child morbidity in Bangladesh: evidence from
a national Bangladeshi sample. Arch Pediatr Adolesc Med
2009;163:700-5. CrossRef
15. Andersson N, Cockcroft A,
Ansari U, et al. Barriers to disclosing and reporting violence
among women in Pakistan: findings from a national household survey
and focus group discussions. J Interpers Violence 2010;25:1965-85. CrossRef
16. Farid M, Saleem S, Karim MS,
Hatcher J. Spousal abuse during pregnancy in Karachi, Pakistan.
Int J Gynaecol Obstet 2008;101:141-5. CrossRef
17. Ali TS, Bustamante-Gavino I.
Prevalence of and reasons for domestic violence among women from
low socioeconomic communities of Karachi. East Mediterr Health J
2007;13:1417-26.
18. Shaikh MA. Domestic violence
against women-perspective from Pakistan. J Pak Med Assoc
2000;50:312-4.
19. Boyle MH, Georgiades K, Cullen
J, Racine Y. Community influences on intimate partner violence in
India: women’s education, attitudes towards mistreatment and
standards of living. Soc Sci Med 2008;69:691-7. CrossRef
20. Ntaganira J, Muula AS, Siziya
S, Stoskopf C, Rudatsikira E. Factors associated with intimate
partner violence among pregnant rural women in Rwanda. Rural
Remote Health 2009;9:1153.
21. Vives-Cases C, Alvarez-Dardet
C, Gil-González D, Torrubiano-Domínguez J, Rohlfs I, Escribà-Agüir
V. Sociodemographic profile of women affected by intimate partner
violence in Spain [in Spanish]. Gac Sanit 2009;23:410-4. CrossRef
22. Seth P, Raiford JL, Robinson
LS, Wingood GM, DiClemente RJ. Intimate partner violence and other
partner-related factors: correlates of sexually transmissible
infections and risky sexual behaviours among young adult African
American women. Sexual Health 2010;7:25-30. CrossRef
23. Rani M, Bonu S. Attitudes
toward wife beating a cross-country study in Asia. J Interpers
Violence 2009;24:1371-97. CrossRef
24. Dhaher EA, Mikolajczyk RT,
Maxwell AE, Kramer A. Attitudes toward wife beating among
Palestinian women of reproductive age from three cities in West
Bank. J Interpers Violence 2010;25:518-37. CrossRef
25. Easton CJ, Weinberger AH,
McKee SA. Cigarette smoking and intimate partner violence among
men referred to substance abuse treatment. Am J Drug Alcohol Abuse
2008;34:39-46. CrossRef
26. Stuart GL, Temple JR,
Follansbee KW, Bucossi MM, Hellmuth JC, Moore TM. The role of drug
use in a conceptual model of intimate partner violence in men and
women arrested for domestic violence. Psychol Addict Behav
2008;22:12-24. CrossRef