COVID-19: evidence for 2-week versus 3-week quarantine
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
LETTER TO THE EDITOR
COVID-19: evidence for 2-week versus 3-week
quarantine
KL Hon, MB, BS, MD1,2; Karen KY Leung, MB, BS, MRCPCH1; Maggie Wang, PhD3; S Zhao, PhD3
1 Department of Paediatrics and Adolescent Medicine, Hong Kong Children’s Hospital, Hong Kong SAR, China
2 Department of Paediatrics, CUHK Medical Centre, The Chinese University of Hong Kong, Hong Kong SAR, China
3 The Jockey Club School of Public Health and Primary Care, Faculty of Medicine, The Chinese University of Hong Kong, Hong Kong SAR, China
Corresponding author: Dr KL Hon (ehon@hotmail.com)
 Full paper in PDF
Full paper in PDF
To the Editor—A new variant of coronavirus disease 2019 (COVID-19, SARS-CoV-2 VUI 202012/01) was
identified in the United Kingdom before Christmas
2020. Preliminary reports suggested that this variant
was up to 70% more transmissible compared with
previous strains in circulation.1 In response, large
parts of London and South East England introduced
the strictest Tier 4 restrictions, where all residents
were asked to remain at home, all non-essential
shops closed and Christmas celebrations cancelled
for many families in the country.2 This new variant
had already been identified in other countries across
Europe and beyond (including Australia, Japan and
Canada).1 3 The Hong Kong SAR Government swiftly
responded by escalating quarantine requirements
for inbound travellers from 14 to 21 days, one of
the strictest quarantine policies around the world
(Table 1 4 5 6 7). It is important to examine the scientific
evidence for the effectiveness of quarantine practices
to reassure citizens, government officials, and law
enforcing personnel.
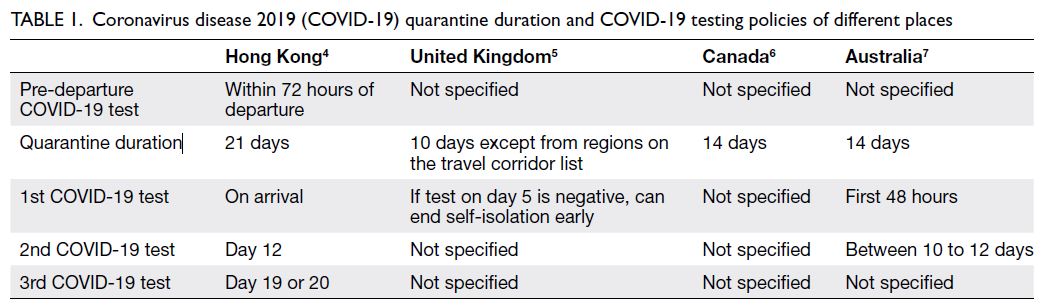
Table 1. Coronavirus disease 2019 (COVID-19) quarantine duration and COVID-19 testing policies of different places
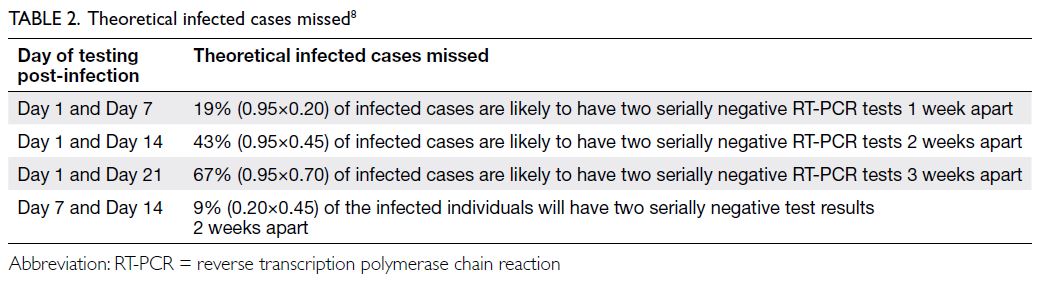
To compare the effectiveness of various
quarantine protocols, a study focusing on infected
individuals and the probability of ‘missing’ such
cases under each protocol based on the evidence available has been conducted (Table 2).8 Serial testing on days 7 and
14 appeared to be the most effective with 91% of
infected individuals identified. On the contrary, the
yield was unsatisfactory for serial testing on days 1
and 14 or 21 with a substantial proportion of positive
cases missed (43% and 67%, respectively).
Nonetheless the likelihood of COVID-19
transmission is not evenly distributed along the
timeline post infection. By applying the known
epidemiological characteristics of COVID-19
transmission (ie, transmission follows a gamma
distribution with mean=5.3 days, standard
deviation=2.1 days, and basic reproduction
number=2.5), we can infer the effectiveness of
different quarantine durations. For example, an
infected individual who has two serially negative
reverse transcription polymerase chain reaction
(RT-PCR) tests 1 week apart who is released on day
7 post-infection would cause infection in around
0.092 secondary cases (2.5×19%×19.3%). In a second
scenario, an infected person with two serially negative
RT-PCR tests 2 weeks apart who is released on day 14
post-infection would lead to 0.001 secondary cases
(2.5×43%×0.1%). In a third scenario that reflects the
latest quarantine changes, an infected individual with two serially negative RT-PCR tests 3 weeks
apart and who is released on day 21 post-infection
would lead to approximately 0.000 secondary cases
(2.5×67%×0.0%). Clearly, the largest reduction in risk
of secondary cases due to imported seed cases can
be achieved through the 2-week policy rather than a
1-week policy of isolation (99% reduction in risk of
secondary cases).
Based on this evidence, it can be concluded
that a protocol of 2 weeks quarantine, not 3, will
miss one infected person for every 1000 infected
persons. Over 8000 reported cases (8425) have been
identified in Hong Kong to date and the majority were
not quarantined at the time of writing in early 2021.
If we apply the policy of quarantine for 2 weeks with
two serial tests, we would have missed eight infected
individuals who would have been identified over the
last 12 months had they been quarantined for 21 days.
Based on scientific evidence, the policy of
3-week quarantine can potentially reduce the risk of introducing this new highly contagious variant. This strict quarantine policy
will come with a very high economic cost, but was
considered as essential to protect the lives of Hong
Kong citizens during the middle of the COVID-19 pandemic in December 2020. In hindsight, our observation provides
important information to guide quarantine policy
about emerging respiratory viral infections with
similar infectivity, basic (and initial) reproduction
number R0 (R-naught), and the current reproduction
number Rt (R at time t).
Author contributions
All authors contributed to the concept or design, acquisition
of data, analysis or interpretation of data, drafting of the
manuscript, and critical revision of the manuscript for
important intellectual content. All authors had full access to
the data, contributed to the study, approved the final version
for publication, and take responsibility for its accuracy and
integrity.
Conflicts of interest
As an editor of the journal, KL Hon was not involved in the peer review process. Other authors have no conflicts of
interest to disclose.
Funding/support
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
1. World Health Organization. SARS-CoV-2 Variant–United Kingdom of Great Britain and Northern Ireland.
2020. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2020-DON304. Accessed 28 Dec 2020.
2. ABC News. London to go into strictest restrictions as
new variant of COVID-19 identified. Available from: https://www.abc.net.au/news/2020-12-15/london-to-get-into-strictest-restrictions-highest-covid-rate/12973596. Accessed 28 Dec 2020.
3. BBC News. Coronavirus: cases of new variant appear worldwide. Available from: https://www.bbc.com/news/world-europe-55452262. Accessed 28 Dec 2020.
4. Hong Kong SAR Government. Quarantine for inbound travellers–frequently asked questions. Available from:
https://www.coronavirus.gov.hk/eng/inbound-travel-faq.html#FAQ7. Accessed 28 Dec 2020.
5. United Kingdom Government. Entering the UK. 2020. Available from: https://www.gov.uk/uk-border-control/ending-self-isolation-early-through-test-to-release. Accessed 27 Dec 2020.
6. Government of Canada. Travel restrictions in Canada.
Mandatory isolation or quarantine. Available from: https://travel.gc.ca/travel-covid/travel-restrictions/isolation. Accessed 27 Dec 2020.
7. Department of Health, Australian Government. Coronavirus (COVID-19) advice for international travellers. Available from: https://www.health.gov.au/news/health-alerts/novel-coronavirus-2019-ncov-health-alert/coronavirus-covid-19-restrictions/coronavirus-covid-19-advice-for-international-travellers. Accessed 27 Dec 2020.
8. Kucirka LM, Lauer SA, Laeyendecker O, Boon D, Lessler J. Variation in false-negative rate of reverse transcriptase polymerase chain reaction–based SARS-CoV-2 tests by time since exposure. Ann Intern Med 2020;173:262-7. Crossref