Hong Kong Med J 2026;32:Epub 13 Apr 2026
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Validation of EuroSCORE II in post–cardiac
surgery patients in a tertiary institution in Hong Kong
Karen HL Ng, MStat1; Kailu Wang, PhD2; Takuya Fujikawa, MD1,3; Micky WT Kwok, MB, ChB, FRCS1,3; Jacky YK Ho, MB, ChB, FRCS1,3; Simon CY Chow, MB, ChB, FRCS1,3; Joyce WY Chan, MB, BS, FRCS1,3; Kevin Lim, MB, ChB, FRCS1,3; Aliss TC Chang, MB, ChB, FRCS1,3; Ivan CH Siu, MB, ChB, MRCS1,3; Randolph HL Wong, MB, ChB, FRCS1,3
1 Division of Cardiothoracic Surgery, Department of Surgery, Prince of
Wales Hospital, Hong Kong SAR, China
2 Centre for Health Systems and Policy Research, The Jockey Club
School of Public Health and Primary Care, Faculty of Medicine, The
Chinese University of Hong Kong, Hong Kong SAR, China
3 Division of Cardiothoracic Surgery, Department of Surgery, The Chinese
University of Hong Kong, Hong Kong SAR, China
Corresponding author: Prof Randolph HL Wong (wonhl1@surgery.cuhk.edu.hk)
 Full paper in PDF
Full paper in PDF
Abstract
Introduction: This study aimed to assess the
discriminatory ability and calibration performance
of the European System for Cardiac Operative
Risk Evaluation (EuroSCORE) II, a widely used risk
prediction tool, in predicting postoperative mortality
among patients undergoing cardiac surgery at Prince
of Wales Hospital (PWH) in Hong Kong.
Methods: Complete data from 4180 patients who
underwent cardiac surgery at PWH between 2013 and
2023 were available for validation of EuroSCORE II
and comparison of its discriminatory ability with the
logistic EuroSCORE. Discriminatory performance
was primarily assessed using the area under the
receiver operating characteristic curve (AUROC).
Calibration was evaluated using the Hosmer–Lemeshow test, coefficient of determination (R2),
and normalised root mean square error (NRMSE).
Results: EuroSCORE II demonstrated strong
discrimination and good calibration for
predicting 30-day mortality in the overall cohort
(AUROC=0.829; Hosmer–Lemeshow P=0.155)
and key subgroups: isolated coronary artery bypass
grafting (CABG) [AUROC=0.847; P=0.113], isolated
valve surgery (AUROC=0.810; P=0.162), and aortic
surgery (AUROC=0.735; P=0.549). More than 85% of
the variation in 30-day mortality (R2) was explained
across these groups. Compared with the logistic
EuroSCORE, EuroSCORE II showed improved
discrimination and calibration, with higher AUROC values and lower NRMSE.
Conclusion: EuroSCORE II demonstrates strong
discriminatory ability and good calibration for
predicting 30-day mortality among patients
undergoing cardiac surgery and within key
subgroups—isolated CABG, isolated valve surgery,
and aortic surgery—in this cohort.
New knowledge added by this study
- The European System for Cardiac Operative Risk Evaluation (EuroSCORE) II demonstrates strong discriminatory ability and good calibration for predicting 30-day mortality among patients undergoing cardiac surgery at Prince of Wales Hospital (PWH) in Hong Kong.
- EuroSCORE II demonstrates improved discrimination and calibration compared with the logistic EuroSCORE in the overall cardiac surgery cohort at PWH.
- Within the aortic subgroup, EuroSCORE II demonstrates statistically significant improvements in discrimination and calibration relative to the logistic EuroSCORE.
- EuroSCORE II represents a reliable risk stratification tool for guiding treatment decisions, identifying high-risk patients and optimising resource allocation.
- Incorporation of additional variables into EuroSCORE II may further enhance predictive accuracy and enable tailored interventions for post–cardiac surgery patients.
Introduction
The Global Burden of Disease Results Tool of
the Institute for Health Metrics and Evaluation
reported that cardiovascular diseases accounted
for approximately 10 383 550 deaths globally in
2017, representing 18.56% of all-cause mortality.1
Cardiothoracic surgery plays an important role in
the treatment of these conditions and in reducing
associated morbidity and mortality. However,
surgery carries inherent risks that vary among
patients, necessitating careful evaluation of risks
and benefits before proceeding. A risk stratification
tool is essential for effective patient triage and the
consent process.
One widely used risk stratification tool is
the European System for Cardiac Operative Risk
Evaluation (EuroSCORE), a specialised scoring
system that provides customised predictions of in-hospital
mortality after cardiac surgery. The tool
assigns scores based on various preoperative risk
factors to stratify patients into different risk categories
(low: EuroSCORE <4%, intermediate: 4-8%, high:
>8%).2 In the UK, in-hospital mortality declined
from 4.0% to 2.8% between 2002 and 2016 following
implementation of EuroSCORE,3 supporting its value
in cardiac surgical risk assessment. The EuroSCORE comprises three versions: the additive EuroSCORE,4
the logistic EuroSCORE,5 and EuroSCORE II.6 In
2012, the Society for Cardiothoracic Surgery in
Great Britain and Ireland recommended the use of
the latest version, EuroSCORE II.6
Prince of Wales Hospital (PWH) in Hong
Kong has adopted the logistic EuroSCORE for risk
assessment since 2007. However, several publications
from different countries have raised concerns
regarding the accuracy of the additive and logistic
EuroSCORE models, leading to the development
of EuroSCORE II.7 8 9 Consequently, EuroSCORE II
has been proposed as the future risk adjustment
tool of the Society for Cardiothoracic Surgery in
Great Britain and Ireland following successful
contemporary validation.6 10 11
Although EuroSCORE II has been widely
used and validated, the underlying data were
predominantly derived from Western populations
undergoing cardiac surgery in Europe and the US.4 12 13 14
Therefore, studies evaluating the performance
of EuroSCORE II in Asian populations remain
limited,15 16 17 and none has been conducted
specifically in Hong Kong. Furthermore, no studies
have compared the performance of the logistic
EuroSCORE and EuroSCORE II in the Hong Kong
population. The present study aimed to address
these gaps.
Moreover, Hong Kong has a higher proportion
of aortic surgery than Western countries. PWH
reported a surge in aortic surgeries, reaching 26%
between 2021 and 2022,18 whereas the UK reported
an aortic surgery prevalence of 3.47% between
2015 and 2016.3 We therefore sought to investigate
whether this variation influences the validity of
EuroSCORE II through subgroup analyses.
The primary objective of this study was to
assess the discriminatory ability and calibration of
EuroSCORE II in predicting postoperative mortality
after the three main index cardiac surgeries (ie,
coronary artery bypass grafting [CABG], valve
surgery, and aortic surgery) at our centre.2 7 8 9 14 15 16 17 19 20 21 22 23 The secondary objective was to compare the
discriminatory ability and calibration of EuroSCORE
II with those of the logistic EuroSCORE in patients
undergoing cardiac surgery.
Methods
Study design and population cohort
This retrospective validation study included patients
(aged ≥18 years) who underwent all types of cardiac
surgery—including CABG, valve surgery (eg, aortic
valve replacement, mitral valve replacement, and
tricuspid valve repair), aortic surgery, isolated or
combined procedures, and other procedures (eg, left
atrial appendage closure) at PWH between 1 January
2013 and 31 December 2023 (inclusive) [Fig]. Because PWH does not perform certain cardiothoracic
procedures—such as paediatric cardiac surgery,
cardiac transplantation, and oesophageal surgery—records for these interventions were unavailable. For
patients who underwent multiple cardiac surgeries
during the same hospital admission, only the first
index procedure was analysed. The minimum sample
size of 225 was calculated based on estimates of area
under the receiver operating characteristic curve
(AUROC) from the literature7 and the estimated prevalence of the outcome (online supplementary Table),7 24 indicating that our primary cohorts for
CABG, valve surgery, and aortic surgery exceeded
the required sample size.
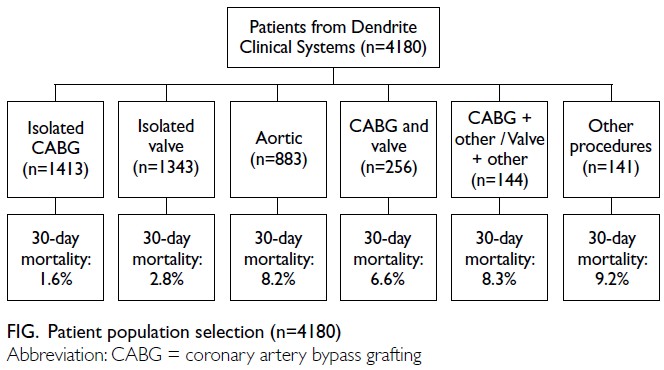
Figure. Patient population selection (n=4180)
Data collection and outcomes
The Dendrite cardiac surgery database (Dendrite
Clinical Systems, Oxford, United Kingdom)25 was
utilised for secondary data collection (Fig). This
database captures clinically relevant information,
including preoperative medical records and
postoperative complications for patients undergoing
cardiac surgery. All key variables required to calculate
EuroSCORE II6 and the logistic EuroSCORE5
were extracted. Mortality, the primary outcome,
was defined as death within 30 days of the index
operation (regardless of place of death), consistent
with previous studies.2 9 14 15 21
Statistical analyses
Cases with missing or incomplete data required
for calculation of EuroSCORE II were excluded
from the analysis. Analyses were performed for
the overall cohort and stratified by individual
cardiac procedure. Complete data were available
for validation of EuroSCORE II and comparison of
its predictive performance with that of the logistic
EuroSCORE for postoperative mortality.
Univariate and multivariate binary logistic
regression analyses were conducted on all relevant
variables included in the EuroSCORE II scale to
identify significant covariates associated with an
increased risk of mortality.
The discriminatory performance of the
predictive models was evaluated using the AUROC;
values of 0.8 or above indicated strong discrimination,
and 1.0 indicated perfect discrimination. Pairwise
comparisons of AUROCs for individual cardiac
procedures were performed using the DeLong test,
with the threshold for statistical significance set at
P<0.05.
Calibration of the predictive model was
evaluated using the Hosmer–Lemeshow goodness-of-fit test and calibration plots, through statistical
and graphical assessment of agreement between
observed and expected event rates within model
subgroups. A P value >0.05 and a regression line
approximating the 45-degree diagonal indicated good calibration, reflecting adequate agreement
between observed and predicted event rates.
Model goodness of fit was further assessed
using the coefficient of determination (R2), which
quantifies the proportion of variance explained by
the model, and the normalised root mean square
error (NRMSE), which measures predictive accuracy
by comparing predicted and observed values,
normalised to the data range. Higher R2 values and
lower NRMSE values indicate better model fit.
Statistical analyses were performed using SPSS
(Windows version 29.0; IBM Corp, Armonk [NY],
United States), Microsoft Excel 2019, and R software
(RStudio, version 2024.04.2).
Results
Patient characteristics
The study cohort comprised 4180 patients (Fig).
Table 1 summarises the characteristics of the
overall cohort and relevant subgroups. The median
age was 63 years (interquartile range, 56-69), and
29.2% (n=1222) were women. Aortic operations
were performed in 21.1% (n=883) of patients and
the majority underwent a single non-coronary
procedure (36.9%, n=1541). For the overall cohort,
the median logistic EuroSCORE value was 5.8
(interquartile range, 2.6-13.7), whereas median
EuroSCORE II value was 2.4 (interquartile range,
1.2-5.3). The institutional 30-day mortality rate for
all cardiac procedures was 4.2%.
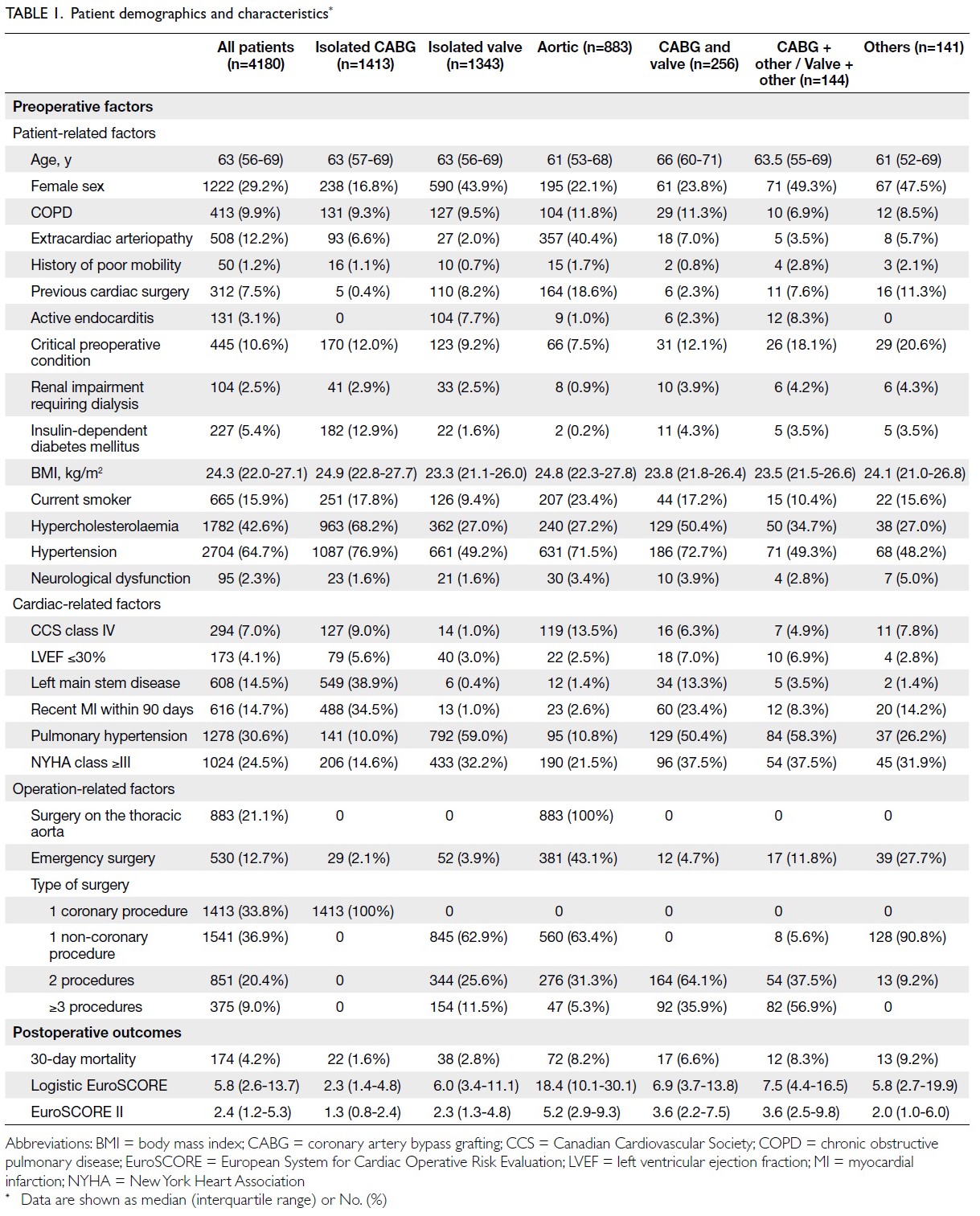
Table 1. Patient demographics and characteristics
Primary outcome
Discriminatory and calibration performance
The AUROC for EuroSCORE II was 0.829, indicating
strong discriminatory ability. The Hosmer–Lemeshow P value for EuroSCORE II was 0.155,
indicating no statistically significant difference
between predicted and observed values (online supplementary Fig a). Accordingly, EuroSCORE II
demonstrated acceptable calibration.
Comparison between logistic EuroSCORE and
EuroSCORE II
EuroSCORE II demonstrated a statistically
significant improvement in discriminatory
performance compared with the logistic EuroSCORE
(DeLong P=0.006). Additionally, EuroSCORE
II showed superior calibration, supported by a
significant Hosmer–Lemeshow test result for the
logistic EuroSCORE (P<0.001). Calibration curves
comparing observed and predicted 30-day mortality
were consistent with these findings, further
indicating better calibration with EuroSCORE II
than with the logistic EuroSCORE. More than 90%
of the variation in 30-day mortality was explained
by both models (R2 for EuroSCORE II=98.7%; R2 for
logistic EuroSCORE=99.1%). Notably, EuroSCORE
II demonstrated a substantially lower NRMSE (5.7%)
than the logistic EuroSCORE (56.4%), indicating
reduced dispersion and relative variability in
predictions (online supplementary Fig a).
Subgroup analysis
Isolated coronary artery bypass surgery
In this subgroup, EuroSCORE II demonstrated
strong discriminatory performance (AUROC=0.847)
and acceptable calibration (Hosmer–Lemeshow
P=0.113). There was no statistically significant
difference in discriminatory performance between
EuroSCORE II and the logistic EuroSCORE (DeLong
P=0.529). However, EuroSCORE II showed better
calibration, supported by a significant Hosmer–Lemeshow test result for the logistic EuroSCORE
(P<0.001) and calibration curves favouring
EuroSCORE. More than 85% of the variation in
30-day mortality was explained by both models
(R2 for EuroSCORE II=87.7%; R2 for logistic
EuroSCORE=91.4%). Compared with the logistic
EuroSCORE (40.6%), EuroSCORE II demonstrated a
lower NRMSE (13.0%), indicating reduced dispersion
and relative variability (online supplementary Fig b).
Isolated valve surgery
In this subgroup, EuroSCORE II demonstrated
strong discriminatory performance (AUROC=0.810)
and acceptable calibration (Hosmer–Lemeshow
P=0.162). There was no statistically significant
difference in discriminatory performance between
EuroSCORE II and the logistic EuroSCORE
(DeLong P=0.160). Nevertheless, EuroSCORE II
demonstrated superior calibration, supported by
a significant Hosmer–Lemeshow test result for
the logistic EuroSCORE (P<0.001) and calibration
curves favouring EuroSCORE II. More than 90%
of the variation in 30-day mortality was explained
by both models (R2 for EuroSCORE II=94.7%; R2
for logistic EuroSCORE=94.4%). Compared with
the logistic EuroSCORE (80.4%), EuroSCORE II demonstrated a lower NRMSE (21.8%), indicating
reduced dispersion and relative variability (online supplementary Fig c).
Aortic surgery
In this subgroup, EuroSCORE II demonstrated
satisfactory discriminatory performance
(AUROC=0.735) and good calibration (Hosmer–Lemeshow P=0.549). It also showed a statistically
significant improvement in discrimination
compared with the logistic EuroSCORE (DeLong
P<0.001). Calibration was also superior, supported
by a significant Hosmer–Lemeshow test result for
the logistic EuroSCORE (P<0.001) and calibration
curves favouring EuroSCORE II. More than 90% of
the variation in 30-day mortality was explained by
EuroSCORE II (R2 for EuroSCORE II=96.1%; R2 for
logistic EuroSCORE=76.6%). EuroSCORE II also
demonstrated a lower NRMSE (6.6%) than the logistic
EuroSCORE (98.8%), indicating reduced dispersion
and relative variability (online supplementary Fig d).
Combined valve and coronary artery bypass
surgery
In this subgroup, EuroSCORE II demonstrated fair
discriminatory performance (AUROC=0.694) and
good calibration (Hosmer–Lemeshow P=0.606).
There was no statistically significant difference in
discriminatory performance between EuroSCORE II
and the logistic EuroSCORE (DeLong P=0.913). Both
models exhibited adequate calibration (EuroSCORE
II P=0.606; logistic EuroSCORE P=0.280) [online supplementary Fig e].
Combined valve or coronary artery bypass surgery
and other procedures
In this subgroup, EuroSCORE II demonstrated
strong discriminatory performance (AUROC=0.862)
and acceptable calibration (Hosmer–Lemeshow
P=0.159). There was no statistically significant
difference in discriminatory performance between
EuroSCORE II and the logistic EuroSCORE (DeLong
P=0.248). However, EuroSCORE II exhibited
superior calibration compared with the logistic
EuroSCORE (Hosmer–Lemeshow P=0.062) [online supplementary Fig f].
Other procedures
In this subgroup, EuroSCORE II demonstrated
strong discriminatory performance (AUROC=0.872)
but poor calibration (Hosmer–Lemeshow P<0.001).
There was no statistically significant difference in
discriminatory performance between EuroSCORE
II and the logistic EuroSCORE (DeLong P=0.626).
Notably, calibration curves favoured EuroSCORE II
over the logistic EuroSCORE (online supplementary Fig g).
Multivariate binary logistic regression
analysis
Furthermore, comparison of EuroSCORE II variables
with multivariable analyses from PWH database
identified ‘dialysis’ as an additional significant
predictor of increased 30-day mortality (adjusted
odds ratio=3.401) among patients undergoing
cardiac surgery (Table 2).
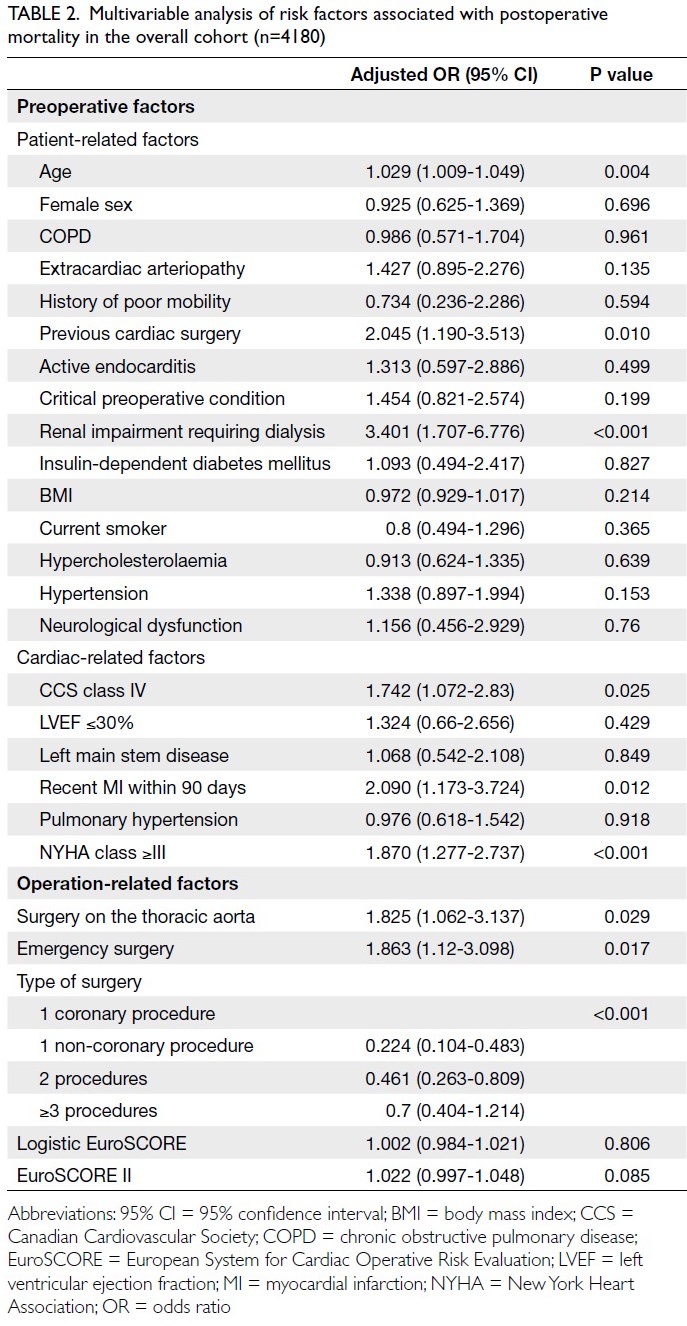
Table 2. Multivariable analysis of risk factors associated with postoperative mortality in the overall cohort (n=4180)
Discussion
In the present study, EuroSCORE II demonstrated
strong discriminatory performance and good
calibration in the overall cohort and three key
subgroups (isolated CABG, isolated valve surgery
and aortic surgery). Moreover, EuroSCORE II
outperformed the logistic EuroSCORE in both
discrimination and calibration across the overall
cohort and these principal subgroups.
Our results are consistent with validation
studies conducted in several European countries
(Italy,26 Greece,27 Serbia,28 Spain,29 and Hungary30),
which demonstrated strong discriminatory
performance (AUROC >0.7) for EuroSCORE II.26 27 28 29 30 31 These findings reaffirm the robust predictive
performance of EuroSCORE II for mortality in
patients undergoing cardiac surgery.
In addition to European populations, our
findings align with those of validation studies
conducted in Asian cohorts.15 16 17 23 Specifically,
Liu et al15 demonstrated strong discriminatory
performance for EuroSCORE II, with an AUROC
of 0.792 in a single-centre setting. This concordance
further supports the consistency and reliability
of EuroSCORE II as a mortality prediction tool in
Asian cardiac surgery populations.
However, Kurniawaty et al19 reported
considerably different findings, demonstrating only
fair discriminatory performance, with evidence of
miscalibration and underprediction in an Indonesian
population. This discrepancy may be attributable to
differences in patient age. Both our cohort and the
European cohorts had substantially higher median
(63 years) or mean (64.6 years)6 ages compared with
the mean age in the Indonesian cohort (44 years)19.
Given the younger age profile and lower prevalence
of risk factors included in the EuroSCORE II
model among Indonesian patients, its predictive
performance may be limited in that population.
Accordingly, these findings may be less generalisable
to the Hong Kong population.
For the overall cohort, EuroSCORE II
demonstrated superior performance in both
discrimination and calibration compared with the
logistic EuroSCORE. This difference may reflect the
tendency of the logistic EuroSCORE to overestimate
mortality risk, particularly in high-risk emergency
patients.10 Consequently, EuroSCORE II appears to
provide more accurate risk stratification than the
logistic EuroSCORE.
For isolated CABG procedures, the
discriminatory performance of EuroSCORE II
was strong in our study, supported by a non-significant
Hosmer–Lemeshow statistic, consistent
with findings from a large UK validation cohort.7
Studies conducted in Finland32 (AUROC=0.852) and
China16 (AUROC=0.762) similarly demonstrated
robust discriminatory performance of EuroSCORE II in predicting operative mortality among high-risk
isolated CABG patients and those undergoing
CABG with or without concomitant major
cardiac surgery. However, a study from Singapore
reported poor discrimination and calibration,
particularly in moderate- and high-risk cohorts.33
Comparable findings were reported in studies from
Indonesia22 and Malaysia,23 which demonstrated fair
discrimination but underestimation of mortality after
isolated CABG. These discrepancies suggest that
additional caution may be warranted when applying
EuroSCORE II in isolated CABG populations.
Differences in demographic characteristics or
study design may contribute to variability in model
performance, warranting further investigation.
For aortic procedures, EuroSCORE II
demonstrated higher AUROC values and more
favourable Hosmer–Lemeshow P values than the
logistic EuroSCORE. Nevertheless, caution is
warranted because the model does not incorporate
specific procedural variables (eg, open surgery vs
minimally invasive approaches) as risk factors, which
may limit precision in mortality prediction for aortic
surgery.7
The adoption of contemporary machine
learning and artificial intelligence techniques, rather
than logistic regression, may offer more effective
modelling approaches for capturing complex,
non-linear interactions among established risk
factors. Furthermore, incorporating the statistically
significant variable identified through multivariate
analysis of the PWH database, specifically dialysis,
into a future EuroSCORE III model may further
enhance its predictive performance.
Strengths
First, the robustness of this validation study is
supported by its substantial sample size (n=4180),
which increases statistical power, enables detection
of smaller effects, and enhances generalisability.
Second, the absence of missing data strengthens
measurement completeness and the credibility of
the validation process, reduces information bias, and
facilitates a more precise evaluation of EuroSCORE
II predictive performance within this large cohort.
Limitations
First, reliance on data from a single institution may
introduce sampling bias. Therefore, multi-centre
analyses should be conducted in future, provided
sufficient resources are available. Second, the
retrospective design limited the study by precluding
long-term follow-up after patient discharge.
Consequently, the analysis did not capture longer-term
outcomes that may be influenced by baseline
EuroSCORE II risk estimates. Additionally, the cohort
demonstrated a skewed distribution across risk
categories, with a substantial proportion (>85.2%) categorised as low or intermediate risk, thereby
limiting generalisability to high-risk populations.
Future research
First, in aortic surgery, the discrepancy in
EuroSCORE II performance observed between
Hong Kong and the UK indicates a need for
further investigation.10 A meta-analysis focusing on
validation of EuroSCORE II in aortic procedures
could help refine risk assessment in this subgroup.
Second, although EuroSCORE II is a valuable risk
stratification tool in cardiac surgery, minimally
invasive cardiac procedures34 and certain established
risk factors (eg, diffuse coronary artery disease and
aortic calcification)15 are not included in the model.
Accordingly, there may be a need for in-depth
evaluation of their relevance to EuroSCORE II
calculation. Third, multi-centre studies would enable
validation of these findings on a broader scale.
Collaboration with the other two cardiac centres
in Hong Kong would enhance generalisability and
support more robust conclusions.
Conclusion
In our cohort, EuroSCORE II demonstrated strong
discriminatory performance and good calibration
for predicting 30-day postoperative mortality among
patients undergoing cardiac surgery. It also shows
superior calibration and comparable or improved
discrimination in the three principal subgroups—isolated CABG, isolated valve surgery, and aortic
surgery—compared with the logistic EuroSCORE.
Accordingly, EuroSCORE II represents a risk
stratification tool superior to the logistic EuroSCORE
and is well suited for use in Hong Kong.
Author contributions
Concept or design: KHL Ng, T Fujikawa, K Wang, RHL Wong.
Acquisition of data: KHL Ng, MWT Kwok, JYK Ho, SCY Chow, JWY Chan, K Lim, ATC Chang, ICH Siu, T Fujikawa, RHL Wong.
Analysis or interpretation of data: KHL Ng, T Fujikawa, K Wang, RHL Wong.
Drafting of the manuscript: KHL Ng, T Fujikawa, K Wang, RHL Wong.
Critical revision of the manuscript for important intellectual content: KHL Ng, T Fujikawa, RHL Wong.
Acquisition of data: KHL Ng, MWT Kwok, JYK Ho, SCY Chow, JWY Chan, K Lim, ATC Chang, ICH Siu, T Fujikawa, RHL Wong.
Analysis or interpretation of data: KHL Ng, T Fujikawa, K Wang, RHL Wong.
Drafting of the manuscript: KHL Ng, T Fujikawa, K Wang, RHL Wong.
Critical revision of the manuscript for important intellectual content: KHL Ng, T Fujikawa, RHL Wong.
All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Conflicts of interest
All authors have disclosed no conflicts of interest.
Acknowledgement
The authors thank Dr Simon KS Yau from Department of Family Medicine of the New Territories East Cluster for his insightful contributions to data interpretation and manuscript revision.
Declaration
This research was presented at The Hospital Authority
Convention 2025 (26 May 2025, Hong Kong).
Funding/support
This research received no specific grant from any funding
agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This research was approved by the Institutional Review Board
of The Chinese University of Hong Kong/Hospital Authority
New Territories East Cluster, Hong Kong (Ref No.: 2024.571).
The requirement for informed patient consent was waived by
the Board due to the retrospective nature of the study.
Supplementary material
The supplementary material was provided by the authors and
some information may not have been peer reviewed. Accepted
supplementary material will be published as submitted by the
authors, without any editing or formatting. Any opinions
or recommendations discussed are solely those of the
author(s) and are not endorsed by the Hong Kong Academy
of Medicine and the Hong Kong Medical Association.
The Hong Kong Academy of Medicine and the Hong Kong
Medical Association disclaim all liability and responsibility
arising from any reliance placed on the content.
References
1. Vervoort D, Swain JD, Pezzella AT, Kpodonu J. Cardiac surgery in low- and middle-income countries: a state-of-the-art review. Ann Thorac Surg 2021;111:1394-400. Crossref
2. Silverborn M, Nielsen S, Karlsson M. The performance of EuroSCORE II in CABG patients in relation to sex, age, and surgical risk: a nationwide study in 14,118 patients. J Cardiothorac Surg 2023;18:40. Crossref
3. Society for Cardiothoracic Surgery in Great Britain and Ireland. Blue Books. Available from: https://scts.org/professionals/reports/resources/. Accessed 10 Sep 2024.
4. Nashef SA, Roques F, Michel P, Gauducheau E, Lemeshow S, Salamon R. European System for Cardiac Operative Risk Evaluation (EuroSCORE). Eur J Cardiothorac Surg 1999;16:9-13. Crossref
5. Roques F, Michel P, Goldstone AR, Nashef SA. The logistic EuroSCORE. Eur Heart J 2003;24:881-2. Crossref
6. Nashef SA, Roques F, Sharples LD, et al. EuroSCORE II. Eur J Cardiothorac Surg 2012;41:734-44. Crossref
7. Chalmers J, Pullan M, Fabri B, et al. Validation of EuroSCORE II in a modern cohort of patients undergoing cardiac surgery. Eur J Cardiothorac Surg 2013;43:688-94. Crossref
8. Zheng Z, Li Y, Zhang S, et al. The Chinese coronary artery bypass grafting registry study: how well does the EuroSCORE predict operative risk for Chinese population? Eur J Cardiothorac Surg 2009;35:54-8. Crossref
9. Yap CH, Reid C, Yii M, et al. Validation of the EuroSCORE model in Australia. Eur J Cardiothorac Surg 2006;29:441-6. Crossref
10. Grant SW, Hickey GL, Dimarakis I, et al. Performance of the EuroSCORE models in emergency cardiac surgery. Circ Cardiovasc Qual Outcomes 2013;6:178-85. Crossref
11. Grant SW, Hickey GL, Dimarakis I, et al. How does EuroSCORE II perform in UK cardiac surgery; an analysis of 23 740 patients from the Society for Cardiothoracic Surgery in Great Britain and Ireland National Database. Heart 2012;98:1568-72. Crossref
12. Roques F, Nashef SA, Michel P, et al. Risk factors and outcome in European cardiac surgery: analysis of the EuroSCORE multinational database of 19030 patients. Eur J Cardiothorac Surg 1999;15:816-22. Crossref
13. Gogbashian A, Sedrakyan A, Treasure T. EuroSCORE: a systematic review of international performance. Eur J Cardiothorac Surg 2004;25:695-700. Crossref
14. Nashef SA, Roques F, Hammill BG, et al. Validation of European System for Cardiac Operative Risk Evaluation (EuroSCORE) in North American cardiac surgery. Eur J Cardiothorac Surg 2002;22:101-5. Crossref
15. Liu PH, Shih HH, Kang PL, Pan JY, Wu TH, Wu CJ. Performance of the EuroSCORE II model in predicting short-term mortality of general cardiac surgery: a single-center study in Taiwan. Acta Cardiol Sin 2022;38:495-503. Crossref
16. Shen L, Chen X, Gu J, Xue S. Validation of EuroSCORE II in Chinese patients undergoing coronary artery bypass surgery. Heart Surg Forum 2018;21:E036-9. Crossref
17. Zhang GX, Wang C, Wang L, et al. Validation of EuroSCORE II in Chinese patients undergoing heart valve surgery. Heart Lung Circ 2013;22:606–11. Crossref
18. Prince of Wales Hospital, The Chinese University of Hong Kong. Cardiac Surgery Report 2021–22. Available from: https://www.surgery.cuhk.edu.hk/cts/Cardiac_Surgery_Report_2021-22.pdf. Accessed 4 Sep 2024.
19. Kurniawaty J, Setianto BY, Widyastuti Y, Supomo S, Boom CE, Ancilla C. Validation for EuroSCORE II in the Indonesian cardiac surgical population: a retrospective, multicenter study. Expert Rev Cardiovasc Ther 2022;20:491-6. Crossref
20. Sembiring YE, Ginting A, Puruhito, Budiono. Validation of EuroSCORE II to predict mortality in post-cardiac surgery patients in East Java tertiary hospital. Med J Indones 2021;30:54-9. Crossref
21. Atashi A, Amini S, Tashnizi MA, et al. External validation of European System for Cardiac Operative Risk Evaluation II (EuroSCORE II) for risk prioritization in an Iranian population. Braz J Cardiovasc Surg 2018;33:40-6. Crossref
22. Zahara R, Soeharto DF, Widyantoro B, Sugisman, Herlambang B. Validation of EuroSCORE II scoring system on isolated CABG patient in Indonesia. Egypt Heart J 2023;75:86. Crossref
23. Musa AF, Cheong XP, Dillon J, Nordin RB. Validation of EuroSCORE II in patients undergoing coronary artery bypass grafting (CABG) surgery at the National Heart Institute, Kuala Lumpur: a retrospective review. F1000Res 2018;7:534. Crossref
24. Riley RD, Ensor J, Snell KI, et al. Calculating the sample size required for developing a clinical prediction model. BMJ 2020;368:m441. Crossref
25. Dendrite Clinical Systems. Databases for hospitals and clinics. Available from: https://www.e-dendrite.com/hospital-systems. Accessed 5 Sep 2024.
26. Paparella D, Guida P, Di Eusanio G, et al. Risk stratification for in-hospital mortality after cardiac surgery: external validation of EuroSCORE II in a prospective regional registry. Eur J Cardiothorac Surg 2014;46:840-8. Crossref
27. Stavridis G, Panaretos D, Kadda O, Panagiotakos DB. Validation of the EuroSCORE II in a Greek cardiac surgical population: a prospective study. Open Cardiovasc Med J 2017;11:94-101. Crossref
28. Nezic D, Spasic T, Micovic S, et al. Consecutive observational study to validate EuroSCORE II performances on a single-center, contemporary cardiac surgical cohort. J Cardiothorac Vasc Anesth 2016;30:345-51. Crossref
29. Garcia-Valentin A, Mestres CA, Bernabeu E, et al. Validation and quality measurements for EuroSCORE and EuroSCORE II in the Spanish cardiac surgical population: a prospective, multicentre study. Eur J Cardiothorac Surg 2016;49:399-405. Crossref
30. Koszta G, Sira G, Szatmári K, Farkas E, Szerafin T, Fülesdi B. Performance of EuroSCORE II in Hungary: a single-centre validation study. Heart Lung Circ 2014;23:1041-50. Crossref
31. Barili F, Pacini D, Capo A, et al. Does EuroSCORE II perform better than its original versions? A multicentre validation study. Eur Heart J 2013;34:22-9. Crossref
32. Biancari F, Vasques F, Mikkola R, Martin M, Lahtinen J, Heikkinen J. Validation of EuroSCORE II in patients undergoing coronary artery bypass surgery. Ann Thorac Surg 2012;93:1930-5. Crossref
33. Luo HD, Teoh LK, Gaudino MF, Fremes S, Kofidis T. The Asian system for cardiac operative risk evaluation for predicting mortality after isolated coronary artery bypass graft surgery (ASCORE-C). J Card Surg 2020;35:2574-82. Crossref
34. Ilcheva L, Risteski P, Tudorache I, et al. Beyond conventional operations: embracing the era of contemporary minimally invasive cardiac surgery. J Clin Med 2023;12:7210. Crossref