Hong Kong Med J 2026;32:Epub 10 Apr 2026
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
CASE REPORT
The first Hong Kong–made three-dimensional–printed sternal implant for metastatic follicular
thyroid carcinoma: a case report
Yan Luk, MB, BS, FRCSEd1; Matrix MH Fung, MB, BS, FRCSEd1; KY Sit, MB, BS, FRCSEd2; Christian Xinshuo Fang, MB, BS, FRCSEd3; Brian HH Lang, MS, FRACS1
1 Division of Endocrine Surgery, Department of Surgery, The University of Hong Kong, Queen Mary Hospital, Hong Kong SAR, China
2 Division of Cardiothoracic Surgery, Department of Surgery, The University of Hong Kong, Queen Mary Hospital, Hong Kong SAR, China
3 Department of Orthopaedics and Traumatology, The University of Hong Kong, Queen Mary Hospital, Hong Kong SAR, China
Corresponding authors: Dr Christian Xinshuo Fang (cfang@hku.hk); Prof Brian HH Lang (blang@hku.hk)
 Full paper in PDF
Full paper in PDF
Case presentation
A 58-year-old female with good past health
presented with an enlarging sternal mass. Computed
tomography revealed a 7-cm osteolytic mass in the
lower sternum with cortical destruction (Fig 1a and b). Core biopsy revealed metastatic follicular thyroid
carcinoma (FTC) with oncocytic cell differentiation.
Ultrasound of the thyroid showed a 1-cm calcified
right thyroid nodule, and fine needle aspiration
cytology suggested an oncocytic cell neoplasm. 18F-fluorodeoxyglucose positron emission
tomography–computed tomography demonstrated
avid uptake in the right thyroid lesion, small
pulmonary metastases and bone metastases, the
largest at the sternum, with small lesions in the right
mandible, left scapula and left tenth rib.
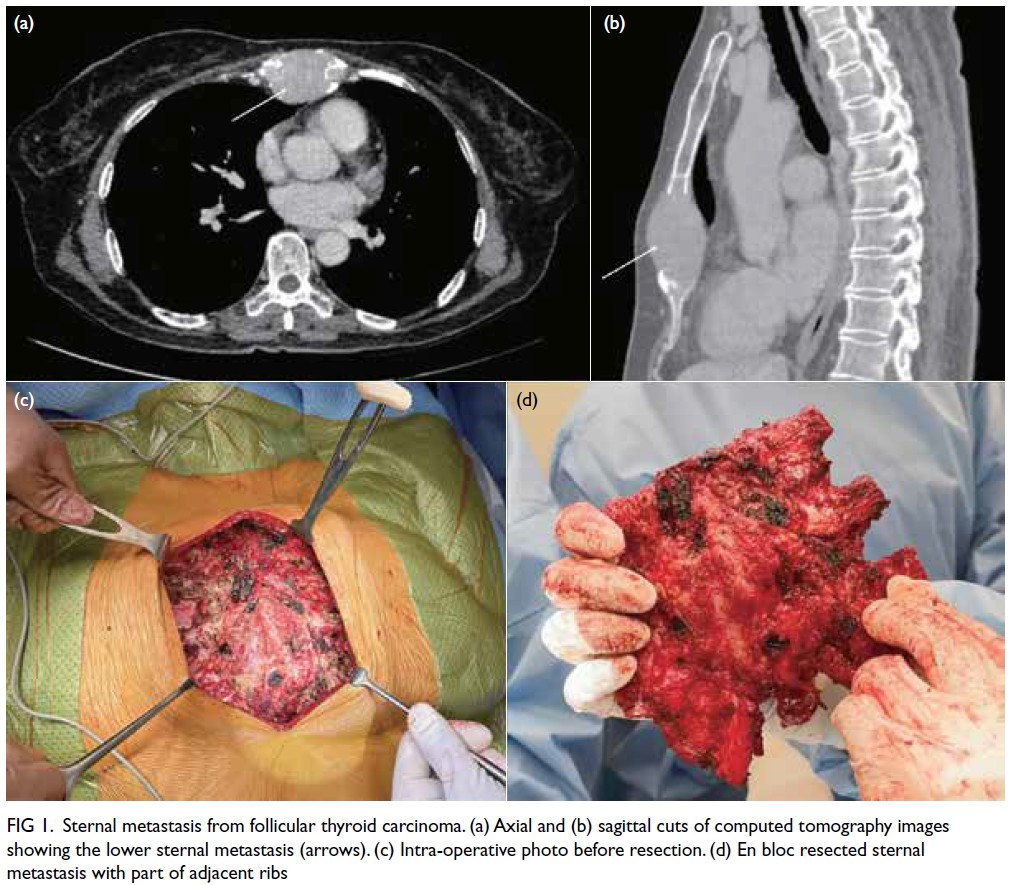
Figure 1. Sternal metastasis from follicular thyroid carcinoma. (a) Axial and (b) sagittal cuts of computed tomography images showing the lower sternal metastasis (arrows). (c) Intra-operative photo before resection. (d) En bloc resected sternal metastasis with part of adjacent ribs
As the large sternal metastasis caused severe
pain, en bloc resection of the sternal tumour was
performed along with the medial ends of the bilateral
anterior ribs (Fig 1c and d). The bony resection
margin was determined preoperatively using the
data from positron emission tomography–computed
tomography and virtual planning software (Mimics;
Materialise, Leuven, Belgium). Reconstruction
was performed with a custom-designed three-dimensional
(3D)–printed titanium alloy implant
(Ti6Al4V Grade 23; Koln 3D Medical, Hong Kong,
China) [Fig 2]. Finite element analysis was performed
to optimise the design for implant longevity by
eliminating stress risers. The 3D-printed surgical
guides ensured precise bone cuts and accurate
implant fitting. The total planning and production
time was 45 days, and the implant weighed 699 g.
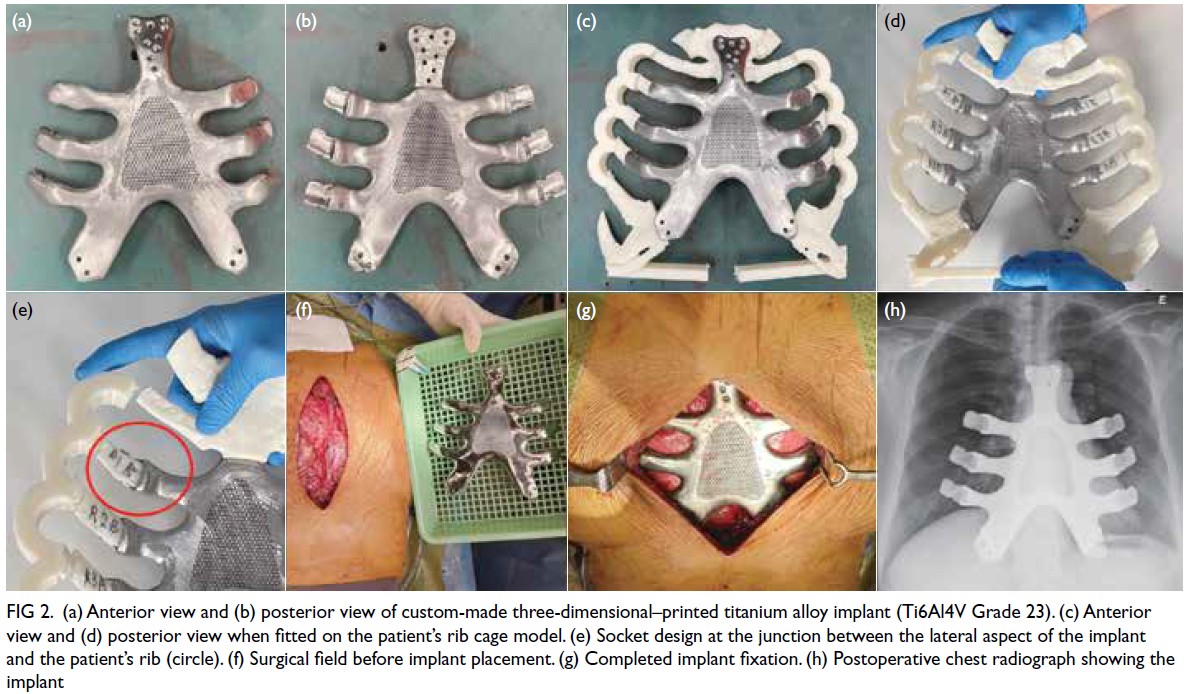
Figure 2. (a) Anterior view and (b) posterior view of custom-made three-dimensional–printed titanium alloy implant (Ti6Al4V Grade 23). (c) Anterior view and (d) posterior view when fitted on the patient’s rib cage model. (e) Socket design at the junction between the lateral aspect of the implant and the patient’s rib (circle). (f) Surgical field before implant placement. (g) Completed implant fixation. (h) Postoperative chest radiograph showing the implant
The superior part of the implant was fixed to the
native manubrium with eight 3.5-mm orthopaedic
angle-stable titanium locking screws (DePuy
Synthes, West Chester [PA], US). The undersurface
of the implant was porous to allow bone ingrowth,
enhancing long-term stability. Laterally, the implant comprised sockets accommodating the native third
to fifth rib stumps, which were further secured with
non-absorbable No. 2 FiberWire sutures (Arthrex,
Naples [FL], US). Inferior to the sixth rib, the
conjoint costal cartilage stump was loosely opposed
to the implant using sutures passed through pre-formed
holes of the implant. A Permacol (Medtronic,
Minneapolis [MN], US) mesh was placed over the
anterior surface of the implant, above which the
muscle flap and skin were closed primarily.
Histopathological examination of the sternal
specimen confirmed metastatic FTC with clear
margins. The patient made an uneventful recovery
and subsequently underwent total thyroidectomy,
which demonstrated multifocal FTC with extensive
capsular invasion.
Postoperatively, the patient received two
courses of radioiodine therapy and continued
bisphosphonate treatment with thyroid-stimulating
hormone suppression. At 1.5 years after the
operation, she had stable disease, was pain-free, and
had resumed work and independent daily activities.
Discussion
To the best of our knowledge, this is the first 3D-printed
sternal implant manufactured in Hong
Kong using medical-grade titanium alloy powder
(TiAl4V Grade 23) by direct metal laser sintering. This custom-made implant represents a novel
reconstructive option that provided excellent
symptomatic relief. It restored the form and strength
of the anterior chest wall while allowing chest wall
motion through its rib-socket design. Previous case
reports and series on resection of sternal metastases
from FTC have utilised alternative reconstructive
methods, including pectoralis major flaps, Marlex
mesh, Gore-Tex mesh, titanium mesh, and acrylic
plates.1
Follicular thyroid carcinoma is the second most
common type of well-differentiated thyroid cancer
after papillary thyroid carcinoma. Although the
presence of distant metastases is a poor prognostic
factor, the 5-year disease-specific survival rate for
metastatic FTC can be as high as 82.2%.2 Given this
considerable life expectancy, balancing oncological
with symptomatic relief is essential for optimal
management.
Radioactive iodine is less effective in treating
bone metastases from differentiated thyroid cancer.
Surgical resection of bone metastases has been
recommended for patients with solitary lesions with
curative intent and for those causing significant
morbidity for symptomatic palliation. Furthermore,
metastasectomy for maximal tumour debulking may
facilitate the effectiveness of radioiodine therapy,
as a higher dose can be concentrated in residual
malignant cells.1
The custom-made implant and tumour
resection plan were based on the patient’s fine-cut
computed tomography images. The implant’s central
mesh structure was not anatomically identical to
the sternum or costal cartilages but still served to
protect the mediastinal structures. The mesh design
reduced implant weight and allowed soft-tissue
ingrowth, theoretically reducing infection risk. Post-processing
involved proprietary heat treatment to
reduce internal stress and material brittleness, while
electropolishing smoothed the surface to reduce
fatigue failure.
A 3D-printed polymer rib cage model was
made to determine a good fit of the implant, and
simulate the implantation process (Fig 2c to e).
The lateral parts of the implant connected to the
bilateral third to fifth ribs via 2-cm–deep socket
design, allowing rib fixture without screws (Fig 2e).
This unique design was adopted from the growing
orthopaedic implants used in children,3 and enabled
free movement of the junctions between the
implant and ribs as well as chest wall expansion and
contraction during breathing.
In previously reported custom sternal implants,
superior fixation was typically achieved using angle-stable
screws in the remaining manubrial bone.4 5
Costal fixation methods varied: most designs used
rigid screws while others incorporated flexible elements at the rib junction, such as polymer
material, spring mechanisms or metal cables and
wires, to enhance implant flexibility.6 One case report
described two paediatric patients with a partially
slidable design, theoretically accommodating
chest cavity growth.7 Nonetheless, fatigue failure
remains a concern across designs, given the human
respiratory cycle of approximately 25 000 breaths
per day and over 250 million cycles over a 30-year
lifespan. Long-term follow-up of patients with
custom sternal prostheses would provide valuable
insight into optimal design and fixation methods.
Our design theoretically reduces metallic stress
and long-term fatigue risk by preserving motion at
the rib-implant junction. Activities of daily living
were gradually resumed, and exercise tolerance
remained unaffected. The surgery successfully
improved our patient’s quality of life, which is vital
given the relatively prolonged survival with FTC.
This implant achieved excellent functional
outcomes and may serve as a model for
reconstruction of large anterior chest wall defects.
With technological advancements in 3D printing,
similar custom-made implants will be more readily
available in the near future, tailored to individual
patient needs. This case demonstrates a novel
treatment for sternal metastasis. Appropriate patient
selection with good premorbid status and reasonable
life expectancy is crucial to ensure maximum benefit
from such surgery.
Author contributions
All authors contributed to the concept or design, acquisition
of data, analysis or interpretation of data, drafting of the
manuscript, and critical revision of the manuscript for
important intellectual content. All authors had full access to
the data, contributed to the study, approved the final version
for publication, and take responsibility for its accuracy and
integrity.
Conflicts of interest
All authors have disclosed no conflicts of interest.
Declaration
This case was presented at the Interesting Case session at
the International Surgical Week 2024 held in Kuala Lumpur,
Malaysia, 26-29 August 2024.
Funding/support
This study received no specific grant from any funding agency
in the public, commercial, or not-for-profit sectors.
Ethics approval
This study was approved by the Institutional Review Board
of The University of Hong Kong/Hospital Authority Hong
Kong West Cluster, Hong Kong (Ref No.: UW 25-049).
Written informed consent was obtained from the patient for
publication of this case report along with the clinical images.
References
1. Batta R, Njoum Y, Deek R, Awad F, Bakri IA, Maree M. Follicular thyroid carcinoma with sternal metastasis: a case report. Int J Surg Case Rep 2023;109:108625. Crossref
2. Sugino K, Kameyama K, Nagahama M, et al. Follicular thyroid carcinoma with distant metastasis: outcome and prognostic factor. Endocr J 2014;61:273-9. Crossref
3. Fassier F. Fassier–Duval telescopic system: how I do it? J Pediatr Orthop 2017;37 Suppl 2:S48-51. Crossref
4. Dzian A, Živčák J, Penciak R, Hudák R. Implantation of a 3D-printed titanium sternum in a patient with a sternal tumor. World J Surg Oncol 2018;16:7. Crossref
5. Liu C, Sun H, Lin F. The application of three-dimensional custom-made prostheses in chest wall reconstruction after oncologic sternal resection. J Surg Oncol 2024;129:1063-72. Crossref
6. Ramírez O, Torres-SanMiguel CR, Ceccarelli M. Design of a compliant sternum prosthesis for improving respiratory dynamics. Prosthesis 2024;6:561-81. Crossref
7. Anderson CJ, Spruiell MD, Wylie EF, et al. A technique for pediatric chest wall reconstruction using custom-designed titanium implants: description of technique and report of two cases. J Child Orthop 2016;10:49-55. Crossref