Hong Kong Med J 2025;31:Epub 10 Dec 2025
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
EDITORIAL
The complementarity of quantitative and
qualitative methods: evaluating educational
activities using mixed methods
HY So, MHPE, FHKAM (Anaesthesiology)1; Stanley SC Wong, MD, FHKAM (Anaesthesiology)2; Abraham KC Wai, MD, FHKAM (Emergency Medicine)3; Albert KM Chan, MHPE, FHKAM (Anaesthesiology)4; Benny CP Cheng, FHKAM (Anaesthesiology)5
1 Educationist, Hong Kong Academy of Medicine, Hong Kong SAR, China
2 Chairman, Scientific Committee, Hong Kong College of Anaesthesiologists, Hong Kong SAR, China
3 Chairman, Research Subcommittee, The Jockey Club Institute for Medical Education and Development, Hong Kong Academy of
Medicine, Hong Kong SAR, China
4 Chairman, Board of Education, Hong Kong College of Anaesthesiologists, Hong Kong SAR, China
5 Honorary Director, The Jockey Club Institute for Medical Education and Development, Hong Kong Academy of Medicine, Hong Kong
SAR, China
Corresponding author: Dr HY So (sohingyu@fellow.hkam.hk)
 Full paper in PDF
Full paper in PDF
In a recent position paper,1 the Hong Kong Academy
of Medicine (HKAM) recommended that both
HKAM and its Colleges establish mechanisms to
evaluate faculty development programmes using
both quantitative and qualitative methods. This
recommendation underscores the importance
of mixed methods approaches in evaluating
educational activities within postgraduate medical
education (PGME). This editorial builds on our
study of the impact of the conjoint workplace-based
assessment (WBA) workshop, published in this
issue of the Hong Kong Medical Journal,2 to
illustrate the effective application of mixed methods
approaches.
Mixed methods combine quantitative and
qualitative approaches to provide a comprehensive
evaluation.3 In healthcare, experimental research
utilising quantitative methods is more familiar; these
methods are equally relevant in medical education.
Quantitative studies rely on measurable data and
statistical analyses to assess the effectiveness of
interventions in numerical terms, such as the
number of trainees achieving a specific competency
level or improvements in assessment scores.
This approach addresses questions such as ‘How
effective was the workshop in enhancing feedback
skills among trainers?’ or ‘What proportion of
trainees demonstrated improved competency after
implementing WBA?’ Quantitative methods are
particularly valuable for investigating cause-and-effect
relationships.4
For descriptive questions about ongoing
events or explanatory questions about how or
why something occurred, qualitative studies are
often the most suitable approach.4 These studies
enhance understanding by exploring experiences,
behaviours, and attitudes, providing insights that cannot be captured through numerical data alone.
This approach is particularly valuable for examining
complex interventions where contextual factors exert
substantial influence. In such situations, adoption of
the CMO model (Context + Mechanism = Outcome)
can be highly effective.5 Qualitative methods (eg,
interviews, focus groups, and observations) enable
the exploration of participants’ perspectives—what they value in an educational intervention,
the challenges they encounter, and areas requiring
improvement. For example, within the context of the
conjoint WBA workshop, qualitative research can
reveal how trainers and trainees perceive WBA and
feedback, their emotional responses, the barriers
they face in effectively integrating WBA into daily
practice, and the factors that facilitate learning
during the workshop.2 Despite the subjective nature
of qualitative research, quality criteria have been
established to ensure its rigour.6
Quantitative and qualitative studies address
distinct research purposes and questions. They
also differ in aspects such as ontology, sampling
methods, and analysis, as summarised in the
Table.7 8 Mixed methods studies combine the
strengths of both approaches, compensating for
the limitations of each. Quantitative data reveal
patterns, whereas qualitative insights provide
essential context and depth, enabling a more
comprehensive understanding. This combination
is particularly important in PGME, where reliance
on quantitative measures alone risks neglecting key
nuances of learner experiences, while qualitative
approaches may lack generalisability. By integrating
both methods, evaluations become more robust
and better suited to inform faculty development,
curriculum enhancement, and improvements to the
clinical learning environment.
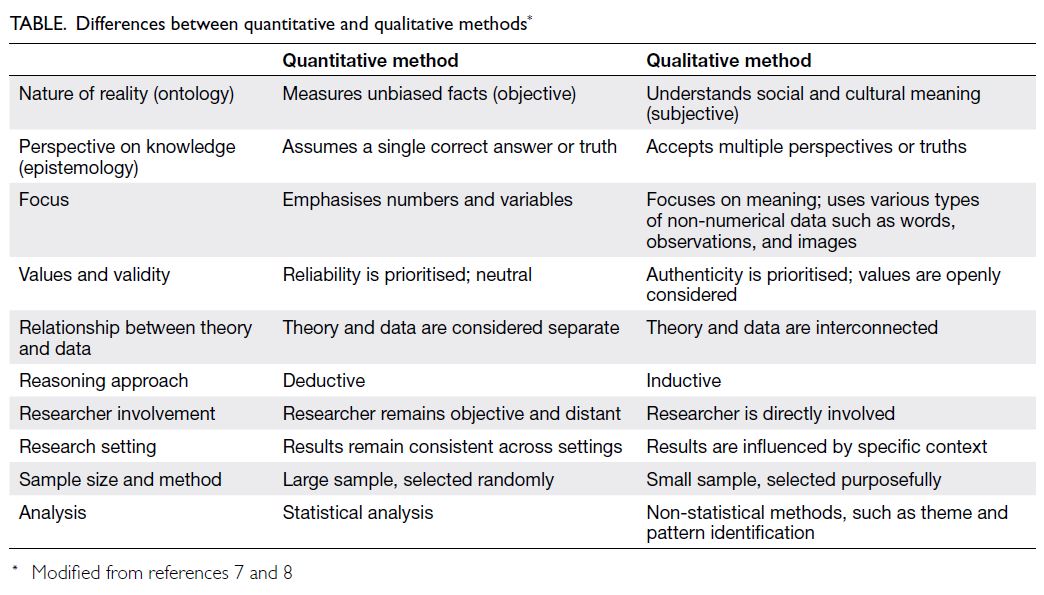
Table. Differences between quantitative and qualitative methods
Four basic designs for mixed methods studies
are commonly used9:
- Exploratory sequential design: Qualitative research is conducted first to explore a topic, guiding a subsequent quantitative study, often for instrument development.
- Explanatory sequential design: Quantitative data are collected first, followed by qualitative research to explain or provide context to the results.
- Triangulation or convergent design: Qualitative and quantitative data are simultaneously collected to compare and contrast findings.
- Longitudinal transformation: Data are collected at multiple points, typically from different populations and using various methods; analysis and integration occur throughout the project.
In the evaluation of the conjoint WBA
workshop, both triangulation and explanatory
approaches were utilised.2 Quantitative outcomes
demonstrated the success of the intervention.
Qualitative findings not only supported these results
but also explained why specific outcomes were
achieved, guiding future refinements.
However, many clinicians are unfamiliar
with qualitative research methods, which limits
their ability to fully engage with mixed methods
evaluations. To address this limitation, the HKAM
position paper also recommended that training
in qualitative evaluation methods be provided to
Fellows responsible for quality assurance.1 The
Research Subcommittee of the Jockey Club Institute
for Medical Education and Development has
collaborated with the Scientific Committee of the Hong Kong College of Anaesthesiologists to develop
a research course that includes both quantitative and
qualitative methods. This course is now in progress
and may subsequently be offered to other Colleges,
thereby enhancing capacity for quality assurance
across specialties.
As PGME increasingly shifts towards
competency-based approaches, evaluations must
evolve to reflect these changes. Mixed methods
offer a practical means of achieving this evolution,
providing a comprehensive understanding of learner
progress and the contextual factors influencing
outcomes.
The integration of mixed methods into
educational evaluations aligns with HKAM’s vision
of a continuous, evidence-based improvement
cycle in PGME. By uncovering both the ‘what’ and
the ‘why’ behind educational outcomes, educators
become better equipped to make informed decisions
that enhance the learning experience and ultimately
improve the quality of care delivered by future
specialists.
Author contributions
All authors have contributed equally to the concept,
development, and critical revision of the manuscript. All
authors had full access to the data, contributed to the
study, approved the final version for publication, and take
responsibility for its accuracy and integrity.
Conflicts of interest
HY So and AKM Chan are co-authors of the article by So et al
(Reference 2), published in the same issue. Other authors have
declared no conflicts of interest.
Funding/support
This editorial received no specific grant from any funding
agency in the public, commercial, or not-for-profit sectors.
References
1. So HY, Li PK, Lai PB, et al. Hong Kong Academy of Medicine
position paper on postgraduate medical education 2023.
Hong Kong Med J 2023;29:448-52. Crossref
2. So HY, Wong EW, Chan AK, et al. Improving efficiency and
effectiveness of workplace-based assessment workshop in
postgraduate medical education using a conjoint design.
Hong Kong Med J 2025 Dec 9. Epub ahead of print. Crossref
3. Maudsley G. Mixing it but not mixed up: mixed methods
research in medical education (a critical narrative review).
Med Teach 2011;33:e92-104. Crossref
4. Eisenhart M. Qualitative science in experimental time. Int
J Qual Stud Educ 2006;19:697-707. Crossref
5. Berwick DM. The science of improvement. JAMA 2008;299:1182-4. Crossref
6. Frambach JM, van der Vleuten CP, Durning SJ. AM last
page. Quality criteria in qualitative and quantitative
research. Acad Med 2013;88:552. Crossref
7. Mehrad A, Zangeneh MH. Comparison between qualitative
and quantitative research approaches: social sciences. Int J
Res Educ Stud 2019;5:1-7.
8. Braun V, Clarke V. Successful Qualitative Research: A
Practical Guide for Beginners. Los Angeles: Sage; 2013.
9. Schifferdecker KE, Reed VA. Using mixed methods
research in medical education: basic guidelines for
researchers. Med Educ 2009;43:637-44. Crossref