Hong Kong Med J 2025;31:Epub 4 Jun 2025
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
CASE REPORT
Adrenal insufficiency due to etomidate inhalation
via electronic cigarettes: three local cases
YK Chung, Cert HKCPaed (PE), FHKAM (Paediatrics)1; YT Cheung, MB, ChB2,3; Cindy SY Chan4, MB, BS, MRCPCH4; CC Wong, MB, BS5; Antony CC Fu, MB, ChB, FHKAM (Paediatrics)4; YY Lam, FRCPCH, FHKAM (Paediatrics)5; CY Lee, FRCP (Edin), FHKAM (Paediatrics)1
1 Department of Paediatrics and Adolescent Medicine, Caritas Medical Centre, Hong Kong SAR, China
2 Hospital Authority Toxicology Reference Laboratory, Hong Kong SAR, China
3 Hong Kong Poison Control Centre, Hospital Authority, Hong Kong SAR, China
4 Department of Paediatrics and Adolescent Medicine, Princess Margaret Hospital, Hong Kong SAR, China
5 Department of Paediatrics, Kwong Wah Hospital, Hong Kong SAR, China
Corresponding author: Dr YK Chung (cyk474@ha.org.hk)
 Full paper in PDF
Full paper in PDF
Case presentations
Etomidate is a non-barbiturate intravenous
anaesthetic agent commonly used in emergency and
critical care settings, due to its rapid onset, short
duration of action, and minimal cardiorespiratory
suppression. Adrenal suppression is a known side-effect.
From April to May 2024, three adolescents
presented to the paediatric departments of local
hospitals with adrenal insufficiency due to etomidate
inhalation via electronic cigarette (e-cigarette)
vaping, a novel form of drug misuse emerging in
Hong Kong.
In Case 1, a 17-year-old male with attention
deficit hyperactivity disorder was admitted with
ketamine cystitis. He had mild hypokalaemia,
hypertension (137/84 mmHg), and a positive urine
toxicology screen by liquid chromatography–tandem mass spectrometry for cocaine, ketamine,
and etomidate (Table). He reported daily vaping
of ‘space oil’ via e-cigarettes for 4 months. Adrenal
insufficiency was diagnosed based on elevated
adrenocorticotropic hormone (ACTH) and a
suboptimal response in a low-dose short Synacthen
test. In Case 2, a 16-year-old male with autistic
spectrum disorder presented with confusion,
insomnia, and unsteady gait after vaping ‘space oil’
weekly for one month. Blood pressure and electrolytes
were normal. Urine toxicology revealed etomidate
and its analogue propoxate. Adrenal insufficiency
was confirmed. In Case 3, a 15-year-old male with
substance abuse–induced psychosis presented
with emotional instability under drug effects. He
reported vaping ‘space oil’ via e-cigarettes weekly
for several months. Blood pressure and electrolytes
were normal. Partial adrenal insufficiency was
diagnosed with borderline results in the low-dose
short Synacthen test. Two patients (Cases 1 and 2)
required regular hydrocortisone replacement. In
Case 1, repeated testing 5 months after cessation of
etomidate revealed persistent adrenal insufficiency, likely due to second-hand smoke exposure from
peers who used etomidate. For Cases 2 and 3, follow-up
tests were planned after etomidate cessation. All
patients received psychiatric follow-up.
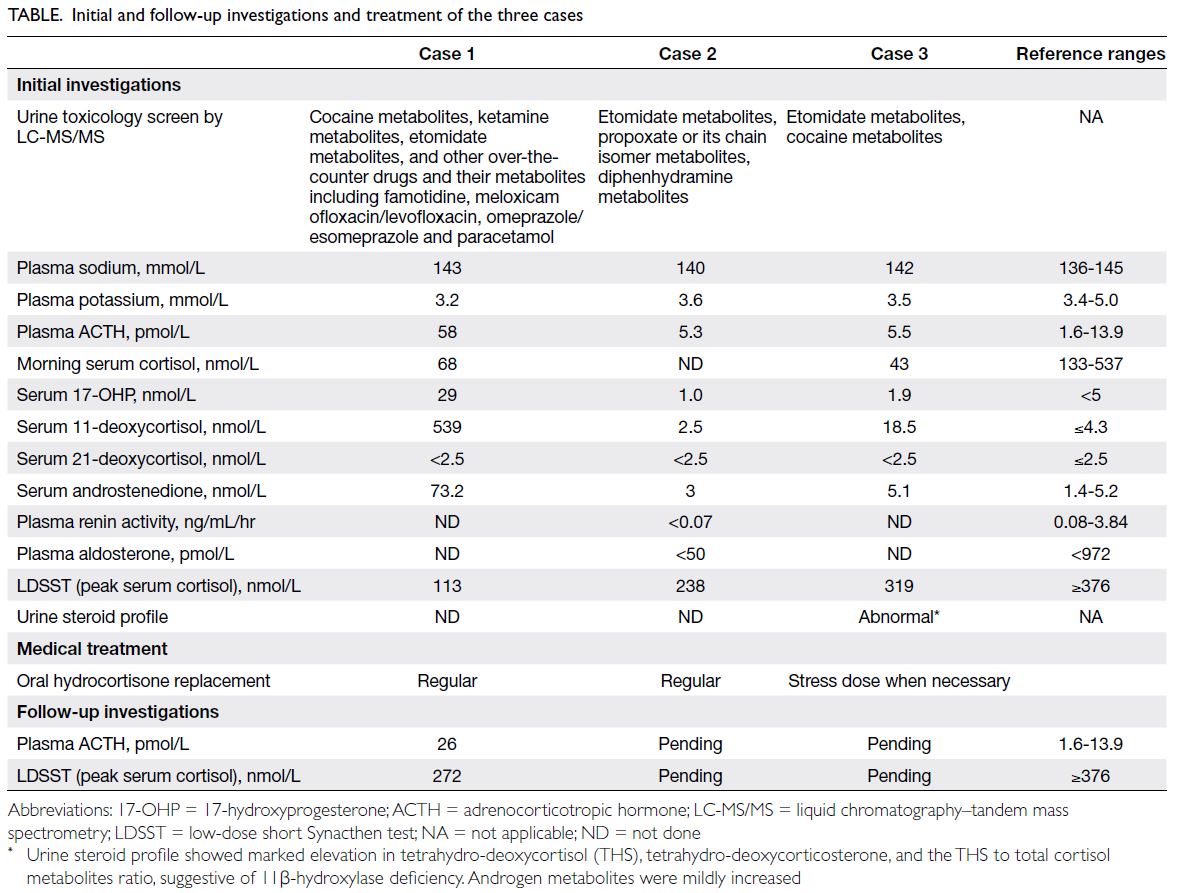
Table. Initial and follow-up investigations and treatment of the three cases
Discussion
This is the first local paediatric report of adrenal
insufficiency associated with etomidate misuse via
e-cigarettes. Since its clinical introduction 40 years
ago, recreational use via the intravenous route has
been rare.1 Nonetheless, its misuse as ‘space oil’
via e-cigarette vaping has surged in Hong Kong
and Mainland China since 2023. e-Cigarette use is
relatively common among adolescents, with a local
survey reporting that 5.3% of secondary school
students have had experience with e-cigarettes.2
From May to December 2024, the Hong Kong
Poison Control Centre recorded 45 cases of ‘space
oil’ misuse presenting to Hospital Authority
emergency departments, with a median patient age
of 17 years.3 Our cases also illustrate that psychiatric
co-morbidities and polysubstance misuse are not
uncommon among adolescent etomidate users.
Knowledge about the pharmacology of inhaled
etomidate is limited since historical studies have
focused on its properties in the context of a single
intravenous bolus or short-duration infusion,4
while inhalation may involve higher doses and
prolonged use. Known toxicities include decreased
consciousness, nausea, vomiting, myoclonus, and
adrenal insufficiency. Respiratory suppression or
bradycardia may develop in overdose. Long-term
neurological and psychological effects, particularly
dependence and withdrawal, remain poorly
characterised.
Etomidate and its analogues, propoxate/isopropoxate, inhibit 11β-hydroxylase, causing
adrenal insufficiency with consequent decreased
cortisol and aldosterone production, and elevated
precursors such as 11-deoxycorticosterone, 11-deoxycortisol, and 17-hydroxyprogesterone (Fig).
Accumulation of deoxycorticosterone, the precursor
to aldosterone, leads to mineralocorticoid excess.
Marked elevation of androstenedione in Case 1 and
urinary androgen metabolites in Case 3 suggested
androgen excess, consistent with a recently reported
local female adult case of hyperandrogenism from
etomidate misuse.5
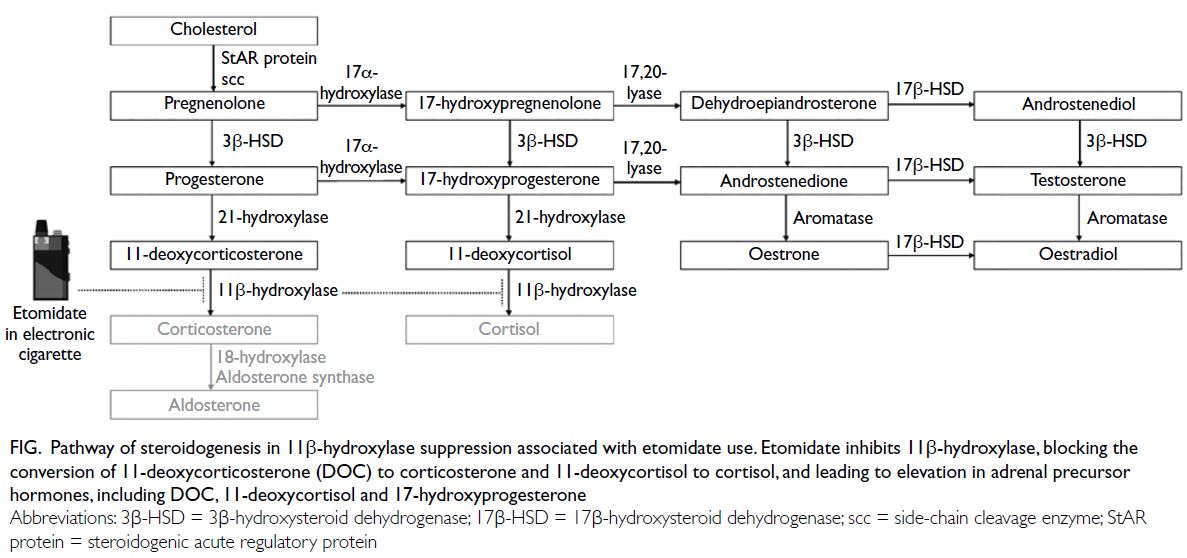
Figure. Pathway of steroidogenesis in 11β-hydroxylase suppression associated with etomidate use. Etomidate inhibits 11β-hydroxylase, blocking the conversion of 11-deoxycorticosterone (DOC) to corticosterone and 11-deoxycortisol to cortisol, and leading to elevation in adrenal precursor hormones, including DOC, 11-deoxycortisol and 17-hydroxyprogesterone
Adrenal suppression from etomidate is dose-dependent
and reversible, lasting 6 to 8 hours after a
single dose and up to 24 to 48 hours with continuous
infusion.4 6 Effects after chronic inhalation are less
clear due to the variable drug content of e-cigarettes
and inconsistent inhalation routes. Adrenal
hyperplasia has been observed on computed
tomography examinations among chronic users,5 7
suggesting possible prolonged ACTH stimulation
due to ongoing adrenal suppression beyond typical
durations in clinical settings.
Etomidate-induced 11β-hydroxylase inhibition
can resemble congenital adrenal hyperplasia due to 11β-hydroxylase deficiency. In addition to
adrenal insufficiency, features of mineralocorticoid
excess include hypertension, hypokalaemia, and
suppression of endogenous renin and aldosterone,
as seen in Case 2. Although mild hypokalaemia
was observed in Case 1, severe hypokalaemia
has been reported.7 Cases 1 and 3 demonstrated
significantly elevated 11-deoxycortisol, while
17-hydroxyprogesterone was normal to mildly
elevated, suggesting the former is a more sensitive
marker of enzyme inhibition, as it is immediately
upstream of the inhibited enzyme (Fig). Urinary
steroid profiling can identify abnormal precursor-to-product ratios. A short Synacthen test should be
performed to confirm adrenal insufficiency. Cases
2 and 3 demonstrated that ACTH may be normal
and cortisol response may be relatively preserved
despite circumstantial evidence of 11β-hydroxylase
inhibition, possibly reflecting less drug exposure or
compensation between periods of drug use.
Given the uncertainty of the duration of adrenal suppression, hydrocortisone replacement
and/or stress dose precautions should be given for
confirmed adrenal insufficiency. Etomidate users
should receive counselling on hydrocortisone’s
role, as it does not mitigate the full spectrum of
etomidate toxicities. After cessation of etomidate,
follow-up testing is recommended to document
adrenal recovery. Persistently abnormal results
should prompt suspicion of ongoing drug use, with
non-classic congenital adrenal hyperplasia due to
11β-hydroxylase deficiency being a rare differential
diagnosis. Our cases highlight the challenges of
achieving complete cessation of drug misuse due
to peer influence and potential dependence. A
multidisciplinary approach should be adopted to
address the complex medical and psychosocial issues
in adolescent etomidate users.
Etomidate and its three analogues—metomidate, propoxate, and isopropoxate—have been listed as dangerous drugs in Hong Kong since February 2025.8 It is expected that more stringent
regulations, along with continued law enforcement
on illegal drug production and distribution, may help
deter etomidate misuse. Public education should
also be strengthened to emphasise that substances
in e-cigarettes are not harmless, even if they are not
traditionally classified as drugs.
Etomidate misuse via e-cigarettes is an
emerging public health issue. Clinicians should
be alert to the risk of adrenal insufficiency among
e-cigarette users, particularly those who present with unexplained hypertension or hypokalaemia.
Additional testing, such as toxicology screening,
11-deoxycortisol measurement, and urinary
steroid profiling may provide supportive evidence.
Further research is warranted to understand the
pharmacological properties and long-term effects of
etomidate misuse.
Author contributions
Concept or design: All authors.
Acquisition of data: YK Chung, YT Cheung, CSY Chan, CC Wong.
Analysis or interpretation of data: All authors.
Drafting of the manuscript: YK Chung.
Critical revision of the manuscript for important intellectual content: All authors.
Acquisition of data: YK Chung, YT Cheung, CSY Chan, CC Wong.
Analysis or interpretation of data: All authors.
Drafting of the manuscript: YK Chung.
Critical revision of the manuscript for important intellectual content: All authors.
All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Conflicts of interest
All authors have disclosed no conflicts of interest.
Funding/support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
The patients were managed in accordance with the Declaration of Helsinki and provided informed consent for all treatments, procedures, and publication.
References
1. Uhm J, Hong S, Han E. The need to monitor emerging
issues in etomidate usage: the misuse or abuse potential.
Forensic Sci Med Pathol 2024;20:249-60. Crossref
2. School-based survey on smoking among students in
2022/23. Health Bureau, Hong Kong SAR Government.
2023. Available from: https://www.censtatd.gov.hk/wbr/B1130201/B11302012024XX01/att/en/78/School-based%20Survey%20on%20Smoking%20among%20Students%20in%202022-23%20-%20Key%20findings_7.pdf. Accessed 15 Aug 2024.
3. Wong IN, Chan CK, Tse ML. Spread of ‘space oil drug’
(etomidate) abuse in Hong Kong and consequent
emergency department presentations. Hong Kong Med J
2025;31:173-4. Crossref
4. Forman SA. Clinical and molecular pharmacology of etomidate. Anesthesiology 2011;114:695-707. Crossref
5. Lau CY, Cheung YT, Han TM, Chung CM, Chong YK,
Chen PL. Acquired 11β-hydroxylase deficiency by inhaled
etomidate and its analogues: a mimic of congenital adrenal
hyperplasia. JCEM Case Rep 2024;2:luae207. Crossref
6. Vinclair M, Broux C, Faure P, et al. Duration of adrenal
inhibition following a single dose of etomidate in critically
ill patients. Intensive Care Med 2008;34:714-9. Crossref
7. Wu W, Xia C, Gan L, Liao S, Yan Y. Etomidate-induced
hypokalemia in electronic cigarette users: two case
reports and literature review. Front Endocrinol (Lausanne)
2024;15:1321610. Crossref
8. Hong Kong SAR Government. Dangerous Drugs
Ordinance (Amendment of First Schedule) Order 2025.
Available from: https://www.elegislation.gov.hk/hk/2025/ln13!en. Accessed 15 Feb 2025.