© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
SPECIAL ARTICLE
Medical history of Hong Kong
Part I: Controlling fertility: the intrauterine device and biopolitics in Hong Kong, 1963-1974
Part I: Controlling fertility: the intrauterine device and biopolitics in Hong Kong, 1963-1974
Carol CL Tsang, BA, PhD
Department of History, School of Humanities, The University of Hong Kong, Hong Kong SAR, China
Corresponding author: Dr Carol CL Tsang (cctsang1@hku.hk)
 Full paper in PDF
Full paper in PDF
In the face of a persistent fertility decline in Hong
Kong, if not globally, it is hard for today’s generation
to imagine that the city’s population was once
subject to state-funded fertility control programmes.
Hong Kong’s official initiative to control fertility
began in 1936, when a group of British obstetricians
and Chinese elites founded the Hong Kong Eugenics
League after American birth-control activist
Margaret Sanger toured the city.1 The League
provided contraceptive advice to working-class
Chinese women in an attempt to eradicate the evils
of abortion and infanticide.2 By 1950, the League
had been reorganised and renamed the Family
Planning Association of Hong Kong (FPAHK), with
the aim of dissociating itself from Nazi eugenics. It
defined fertility control as a conscious choice, and
aligned itself more closely with similar organisations
worldwide.3 Although the FPAHK’s early aims
encompassed a wide range of services including birth
control, infertility treatment, and family counselling,
its major mission was to advise and provide free
or low-cost contraceptives to Chinese immigrants. Before contraceptive pill became available in Hong
Kong in the late 1960s, the birth-control methods
promoted to immigrants comprised condoms, female
and male sterilisation, and the intrauterine device
(IUD). As early condoms were not user-friendly and
sterilisation was irreversible, most family planners
encouraged working-class women to opt for the
IUD, a long-acting reversible contraception. This
gave women prime responsibility for fertility.
In Hong Kong, the IUD became popular
only after 1963, when the Lippes Loop (Fig 1) was
introduced to replace the platinum IUD that could
easily scratch the uterus. The Lippes Loop, named
after American gynaecologist Jack Lippes, was
claimed by its inventor to be ‘cheap, convenient, and
cancer-free’.4 A flexible plastic device that, in later
versions, contained copper, it remained effective
for up to 20 years once fitted by a doctor. Requiring
a check-up every 6 months, the primary targets of
the Lippes Loop were women with several children,
working women, and those living in crowded
tenements. By September 1964, the Population
Council had granted the FPAHK an unconditional
licence to manufacture the Lippes Loop. By 1965,
the FPAHK had fitted the Loop in nearly 30 000
local women free of charge. Before the pill became
popular in Hong Kong in the late 1960s, the IUD was
the most common contraceptive, particularly among
squatter patients who could not attend clinics for
supplies because of their full-time work.5
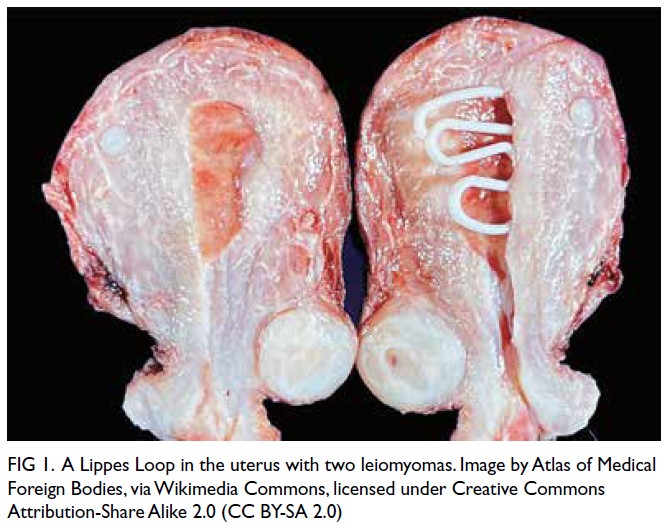
Figure 1. A Lippes Loop in the uterus with two leiomyomas. Image by Atlas of Medical Foreign Bodies, via Wikimedia Commons, licensed under Creative Commons Attribution-Share Alike 2.0 (CC BY-SA 2.0)
Unlike existing scholarship on the refugee
influx in the 1950s and the FPAHK’s ‘Two is Enough’
campaign of 1975,6 the story of the IUD is less about
depopulation in early post-war Hong Kong. Birth
rates had already begun to decline: Hong Kong’s
birth rate fell from 35.5 per 1000 population in 1961
to 25.8 per 1000 population in 1966—a decline of
27%.7 Amid the rising popularity of the contraceptive
pill and concerns over IUD side-effects, the
number of IUD users began to drop as early as
1966. Nonetheless, despite global health scares
surrounding the IUD, Hong Kong family planners
continued to invest resources in maintaining the
device for a specific group of women: those who
were poor, uneducated, and perceived as unable to make their own reproductive decisions.
This article is the first historical study of the
politics of the IUD in Hong Kong. Over the past
decades, research on IUD use in the Global South
has remained scarce, even though most users live
in the region. In the 2010s, the IUD was the second
most prevalent method of fertility control in the
Global South, after female sterilisation, and ranked
fourth in the Global North, after the pill, condoms,
and female sterilisation.8 Today, the IUD is the
most popular method of fertility control in Global
South countries such as China, Vietnam, and North
Korea, and has high adoption in Global North areas
including France, Scandinavia, and the US.9 Scholars
from the Global North have been the strongest
opponents of the device. Feminist historian Andrea
Tone described the IUD as a ‘one-stop birth control’.10
It worked because ‘women could not control it’.11
In Hong Kong in the 1960s, the IUD was a
biopolitical tool that technologically ‘guaranteed
female passivity at every stage of the reproductive
process’.12 It upheld physician authority in the
management of female reproduction and rendered
female users a monolithic group: poor, uneducated,
and irresponsible in managing their own reproduction.
As in the US, the IUD carried strong class and racial
overtones. Most IUD users were women of Chinese
origin who were poor, uneducated, or illiterate, and
living in squatter areas. Hong Kong developed one of
the most successful IUD programmes, drawing the
attention of Alan Guttmacher, president of Planned
Parenthood. Guttmacher compared his observation
of IUD insertions in Hong Kong to ballet: ‘The
best IUD manipulator I have ever observed was in
Hong Kong.... [Dr Wong’s] record was seventy-five
insertions in three hours[,]... that is one every two
minutes and twenty-four seconds. Dr Wong kept
three nurses busy helping her. One was supervising
the removal of the panties of the next patient, the
second nurse soothed the brow of the patient on the
table and the third passed instruments to Dr Wong.
I have never seen such graceful hands, such exquisite
economy of finger movement; there wasn’t a false
motion. I regret that I am not a choreographer, for
a ballet of IUD patients with the ballerina making
Dr Wong’s finger and hand movements would be
a sensation’.13 In Guttmacher’s ballet, these poor,
uneducated women in Hong Kong were reduced
to ‘identical, submissive parts’, passing along ‘the
continuous IUD-insertion assembly line’.14
Hong Kong family planners did not promote
the IUD in isolation. They relied heavily on foreign
aid. During the 20th century, family planners in East
Asia partnered with external agents to advance their
demographic goals. They were not passive recipients
of assistance. Rather, they actively shaped policies
to address local needs.15 The same applied to the
FPAHK. Since its inception, the FPAHK received financial support from the British Commonwealth,
including the Unitarian Service Committee
of Canada and Cambridge Women’s Welfare
Association.16 By the mid-1960s, four IUD clinics in
Hong Kong’s resettlement estates were funded by
Oxfam, a British-funded charity focusing on poverty
relief.17
Above all, the US was the FPAHK’s most
fervent supporter in exerting geopolitical influence
in Asia during the Cold War. Since the early 1960s,
the American Friends Service Committee had
financed the employment of FPAHK field workers
and birth-control clinics.18 In 1966, the American
social demographer Ronald Freedman, head of
the University of Michigan Population Studies
Centre, began collaborating with the FPAHK.
One of his major contributions was to support the
FPAHK’s IUD project. The FPAHK opened its first
intrauterine contraceptive device clinic in 1963 to
provide IUDs to women free of charge.19 By 1964,
around 10 000 IUD insertions had been completed.20
In 1965, FPAHK President Daphne Chun set a target
of fitting 30 000 IUDs in local women free of charge,
with actual insertions reaching 29 651.21 Freedman
supported the FPAHK’s IUD campaign for women
over 35 years of age, but the public began to raise
concerns about possible side-effects, such as ectopic
pregnancy.22
Chun, a renowned obstetrician and the first
Chinese Professor of Obstetrics and Gynaecology
at The University of Hong Kong, was the main
driver of the IUD programme. Having grown up
in Hong Kong and received her education at The
University of Hong Kong, Chun understood the
city’s challenges intimately. In 1963, she compared
the IUD and contraceptive pill by describing Hong
Kong’s dire situation, pledging to ‘find a method
which is economical, harmless, effective, convenient
and acceptable to the majority of our people, who are
poor and housed in quarters shared with others’.23
Costing only 6.5 Hong Kong cents annually and
associated with a low dropout rate owing to its
long-acting nature, the IUD was hailed by Chun as
superior to oral pills, which cost as much as HK$3 a
month and relied on a woman’s compliance.24
Chun’s confidence in the IUD led to a rapid
expansion of services. By 1966, 28 of the 46 female
birth-control clinics offered IUDs. Contraceptives
were usually provided based on economic need and
family size, and IUD insertions were performed
free of charge.25 Nonetheless, success was short-lived.
From 1966 onwards, the number of new IUD
patients dropped considerably. The FPAHK initially
attributed this to six cases of ectopic pregnancy,26
and later to the 1967 Riots.27 Yet family planners
also noted evidence of women’s growing agency:
‘… they usually come on the recommendation of a
friend who has used the method successfully. Many of these women do change to newer methods later’.28
Global efforts to promote the IUD among
users in the Global South, including Hong Kong,
particularly among women with more than four
children, were nonetheless increasing.29 In 1968, the
World Health Organization, under the International
Fertility Research Programme, conducted a medical
trial of the Dalkon Shield (Fig 2) in Hong Kong,
inserting the device into 1200 women.30 Three years
later, over 10 000 women were fitted with the Dalkon
Shield at FPAHK clinics. The Dalkon Shield’s unique
design distinguished it from previous IUDs, but its
multifilament strings and side fins were suspected
of inducing pelvic inflammatory infection, uterine
perforation, and spontaneous septic abortion, as well
as being linked to at least four deaths in the US.31
The FPAHK stopped inserting the device in 1974 and
issued a recall for its removal due to safety concerns.
To this day, it remains unclear whether any local
women claimed damages, largely because of their
low literacy levels. In 1974, the FPAHK enlisted local
women as volunteers to test the still-experimental,
American-made Alza-T.32
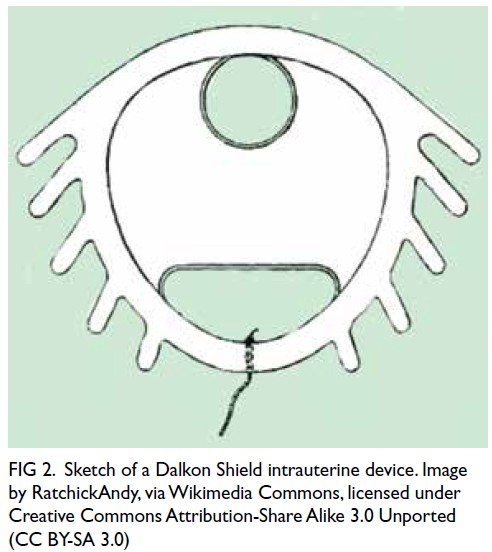
Figure 2. Sketch of a Dalkon Shield intrauterine device. Image by RatchickAndy, via Wikimedia Commons, licensed under Creative Commons Attribution-Share Alike 3.0 Unported (CC BY-SA 3.0)
The silence surrounding the Dalkon Shield
in Hong Kong, despite the global health scare, is
striking. In 1974, FPAHK President Ho-kei Ma,
who succeeded Chun, described numerous cases in
her research on Hong Kong’s experience in which
the Dalkon Shield had perforated the uterine wall,
conjecturing ‘whether the fins on the sides of the
Shield help it to erode into the uterine wall’.33 This
description invites us to reflect on the users’ passivity
and their silence.
The story of the IUD in Hong Kong reveals
how family planning technologies stratified society.
Under the guise of women’s reproductive choice,
the IUD became a means through which physicians,
state actors, and international organisations exerted
authority over poor, working-class women’s bodies.
The persistent use of IUDs between 1963 and
1974 among this marginalised group suggests that
the project was not about managing population
growth, but about determining which women’s
reproductive futures mattered to the modernising
city—a critical reflection that informed the city’s
medical and scientific progress.34 The near silence
in local historical memory surrounding the Dalkon
Shield, coupled with the absence of legal claims or
compensation for affected women, underscores
how the consequences of this biopolitical project
continue to be absorbed silently by those with the
least power to contest it.
Notes
1. The Family Planning Association of Hong Kong. Annual Report 1966-7. Hong Kong: The Family Planning Association of Hong Kong; 1967: 6.
2. Hong Kong Eugenics League. Annual Report 1937-1938. Hong Kong: South China Morning Post; 1938: 2-3.
3. The Family Planning Association of Hong Kong. Annual Report 1951. Hong Kong: The Family Planning Association of Hong Kong; 1951: 2.
4. Wah Kiu Yat Po. 1964 April 5: 10.
5. The Family Planning Association of Hong Kong. Annual Report 1962-3. Hong Kong: The Family Planning Association of Hong Kong; 1963: 27.
6. Tsang CCL. ‘Two is enough’: class, gender and the nuclear family ideal in Cold War Hong Kong. Cold War Hist 2025 Oct 5. Epub ahead of print. Crossref
7. Refer to Note 1: 5, 31.
8. Takeshita C. The Global Biopolitics of the IUD: How Science Constructs Contraceptive Users and Women’s Bodies. 1st ed. Cambridge, Mass: The MIT Press, 2011. Crossref
9. Population Division, United Nations. World Contraceptive Use 2024. Available from: https://www.un.org/development/desa/pd/data/family-planning-data. Accessed 17 Mar 2026.
10. Tone A. Violence by design: contraceptive technology and the invasion of the female body. In: Bellesiles MA, editor. Lethal Imagination: Violence and Brutality in American History. New York: New York University Press; 1999: 384.
11. Refer to Note 10: 381-2.
12. Refer to Note 10.
13. Refer to Note 10.
14. Refer to Note 10.
15. DiMoia JP. “Counting one’s allies”: the mobilisation of demography, population, and family planning in East Asia, late 1920s–present. East Asian Sci Technol Soc 2016;10:355-76. Crossref
16. The Family Planning Association of Hong Kong. Silver Jubilee Report. Hong Kong: The Family Planning Association of Hong Kong; 1975: 22.
17. The Family Planning Association of Hong Kong. Annual Report 1965-6. Hong Kong: The Family Planning Association of Hong Kong; 1966.
18. Refer to Note 17.
19. Refer to Note 5.
20. The Family Planning Association of Hong Kong. Annual Report 1964-5. Hong Kong: The Family Planning Association of Hong Kong; 1965.
21. Refer to Note 1.
22. Refer to Note 1.
23. The Family Planning Association of Hong Kong. Annual Report 1963-4. Hong Kong: The Family Planning Association of Hong Kong; 1964: 9.
24. Refer to Note 23: 11.
25. Refer to Note 17: image 7178.
26. Refer to Note 1: 17.
27. The Family Planning Association of Hong Kong. Annual Report 1967-8. Hong Kong: The Family Planning Association of Hong Kong; 1968: 21.
28. Refer to Note 27: 22.
29. Mauldin WP, Nortman D, Stephen FF. Retention of IUDs: an international comparison. Stud Fam Plann 1967;1:1-12. Crossref
30. South China Morning Post. 1980 May 6: 19.
31. Dalkon Shield. Britannica. Available from: https://www.britannica.com/science/Dalkon-Shield. Accessed 17 Mar 2026.
32. South China Morning Post. 1974 Mar 12: 6.
33. Ma HK, Wei M, Luk KF. The Hong Kong experience in the use of the Dalkon Shield. Contraception 1974;10:113-25. Crossref
34. Sinha R. Medical history of Hong Kong. Introduction—anatomy of a city: why Hong Kong’s history of medicine matters now. Hong Kong Med J 2026;32:75-8. Crossref