Hong Kong Med J 2023 Feb;29(1):57-65 | Epub 9 Feb 2023
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE (HEALTHCARE IN MAINLAND CHINA)
Assessment of healthcare quality among village
clinicians in rural China: the role of internal work motivation
Q Gao, PhD; L Peng, MSc; S Song, MSc; Y Zhang, MSc; Y Shi, PhD
Center for Experimental Economics in Education, Shaanxi Normal University, Xi'an, China
Corresponding author: Prof Y Shi (shiyaojiang7@gmail.com)
 Full paper in PDF
Full paper in PDF
Abstract
Introduction: The quality of primary care is
important for health outcomes among residents
in China. There is evidence that internal work
motivation improves the quality of healthcare
provided by clinicians. However, few empirical
studies have examined the relationship between
internal work motivation and clinical performance
among village clinicians in rural China. This study
was performed to evaluate healthcare quality among
village clinicians, then explore its relationships with
internal work motivation among those clinicians.
Methods: We collected survey data using a
standardised patient method and a structured
questionnaire. We observed 225 interactions
between standardised patients and village clinicians
from 21 counties in three provinces. We used logistic
regression models to analyse the relationships
between work motivation and healthcare quality,
then conducted heterogeneity analysis.
Results: Healthcare quality among village clinicians
was generally low. There was a significantly positive
correlation between internal work motivation and healthcare quality among village clinicians (P<0.1).
Additionally, the positive effect of internal work
motivation on healthcare quality was strongest
among clinicians who received financial incentives
and had a lighter workload (fewer patients per
month) [P<0.1].
Conclusion: Healthcare quality among village
clinicians requires urgent improvement. We
recommend implementing financial incentives to
stimulate internal work motivation among village
clinicians, thus improving their clinical performance.
New knowledge added by this study
- Internal work motivation was positively correlated with healthcare quality among village clinicians in rural China.
- The positive correlation was strongest among clinicians who received financial incentives and had a lighter workload (fewer patients per month).
- Healthcare quality among village clinicians in rural China should be enhanced by improving their internal work motivation.
- Interventions that include financial incentives should be implemented to strengthen the positive effect of internal work motivation on healthcare quality among clinicians.
Introduction
Village clinics, the first tier of rural health systems
in China, are responsible for preventing and treating
common diseases among rural residents.1 2 However,
the quality of healthcare provided by village clinicians
may be unsatisfactory in rural China.3 4 Village
clinicians generally have a low level of education
and limited medical qualifications.4 There is some
evidence that, among village clinicians, the first
records of formal schooling are primarily vocational
school degrees; most (84.3%) of these clinicians only have the basic medical certification necessary to
practise medicine in rural areas.5 Moreover, despite
limited empirical evaluation, available data indicate
that rural primary clinicians have low diagnostic
quality and provide poor management of chronic
diseases.6 A 2012 study in Shaanxi Province revealed
that 41% of diagnoses were incorrect; treatments
were considered correct or partially correct in 53%
of clinician-patient interactions.5 A systematic
review of 24 studies between 2000 and 2012 showed
the rate of antibiotic use in rural clinics was much higher than the rate recommended by the World Health Organization.7 8
The Chinese Government has recognised
the need to strengthen primary healthcare in rural
areas. To improve health among rural residents, the
government has recently issued multiple policies
that are intended to improve service capacity within
primary medical systems.9 10 For example, to improve
clinical knowledge among village clinicians, several
government departments jointly implemented a plan
in 2013, which focused on the provision of continuing
education for clinicians.11 In 2019, the Basic Medical
and Health Promotion Law of the People’s Republic
of China emphasised the need to support the
development of primary medical institutions and
implement various policies that would improve
primary medical service capabilities.12
Although improvements in internal work
motivation among village clinicians may help to
enhance their medical performance, few empirical
studies have examined the relationship between
these two characteristics among village clinicians
in rural China. Theory-focused researches indicate
that internal work motivation is important for
improvements to clinician performance.13 14 Other
theory-based researches in China have suggested that
clinicians with higher internal motivation are more
likely to deliver higher-quality work.15 16 Quantitative
analyses of clinician behaviour, primarily conducted
in other countries, have also revealed positive effects
of internal work motivation on healthcare quality
and work performance of clinicians.17 18 19 To our
knowledge, empirical studies of work motivation in China have primarily focused on individuals in
business careers and similar occupations; few have
considered groups of clinicians.20 21 22 Thus, there
have been few empirical studies involving village
clinicians in rural China.
This study explored the relationship between
internal work motivation and healthcare quality
among village clinicians in rural China. First, using
a standardised patient method and questionnaire
interviews, we evaluated healthcare quality and
internal work motivation among village clinicians.
Second, we examined the relationships between
internal work motivation and healthcare quality
among village clinicians. Third, we conducted
heterogeneity analysis with a focus on clinician
workload and financial incentives.
Methods
Sampling and data collection
Our study sampling was conducted in the rural
areas of three prefectures, each located in one of
the following three provinces: Sichuan, Shaanxi, and
Anhui. Representative samples were selected using a
multi-level random method. First, 21 sample counties
were randomly selected from the sample prefectures.
Next, 10 townships from each sampled county were
randomly chosen as sample townships; 209 sample
townships were selected because one sample county
contained only nine townships. Then, one village
was randomly selected from each township. Finally,
all village clinics in the sample village were included;
one standardised patient interaction was completed
in the sample village.
We conducted two sets of surveys to collect
data regarding basic characteristics, internal
work motivation, and healthcare quality among
village clinicians in 2015. In the first set of surveys,
we primarily gathered information regarding
the characteristics of village clinics and village
clinicians. Specifically, we used a facility structured
questionnaire to enquire about the value of each
sample clinic’s medical instruments and institutional
net income in 2014 (both in Renminbi [RMB]), and
length of daily lunch break (hours). We recorded
the following characteristics of sample village
clinicians: age, gender, level of education and clinical
qualifications, duration of service, monthly salary
(in RMB), number of training days in 2014, clinician
workload (mean number of patients per month),
mean duration of consultation per patient (minutes),
and any financial incentives. Additionally, we asked
village clinicians to respond to questions regarding
internal work motivation.
In the second set of surveys, we used a
standardised patient method to evaluate the
quality of healthcare provided by sample village
clinicians. This method avoids problems such as
the Hawthorne effect and recall bias, accurately assesses healthcare quality among clinicians, and
is widely used in other countries.23 24 We recruited
63 individuals (ie, standardised patients; 21 in each
province) to present three predetermined disease
cases of diarrhoea, tuberculosis, and unstable angina
in a standardised manner. Generally, we randomly
allocated one standardised patient to each sample
clinic to report a case that had been randomly
selected prior to allocation.
Measurement of healthcare quality
We evaluated the quality of healthcare provided
by village clinicians using three indicators: process
quality, diagnostic accuracy, and treatment accuracy.
We assigned a process quality value of 1 to clinicians
who completed more than the mean percentage of
suggested items, indicating a high-quality enquiry
process. Otherwise, the process quality value was 0.
Regarding diagnostic and treatment accuracies, we
assigned a value of 0 to an ‘incorrect’ result, based
on predetermined criteria. Otherwise, ‘correct’ or
‘partly correct’ results were assigned an accuracy
value of 1. The treatment was also considered correct
if the clinician referred the patient to a higher-level
hospital.
Measurement of internal work motivation
According to Amabile and Mueller,25 an individual’s
work motivation is defined as internal work
motivation if it originates from love and interest. The
internal motivation instrument in our study included
four items, such as ‘because I like what I do for a living'.
The responses of four items were rated on a 7-point
Likert-type scale, ranging from 1 = strongly disagree
to 7 = strongly agree. In this study, we assigned a
value of 0 to responses indicating disagreement or
neutrality (with original score of 1-4) and a value of
1 to responses indicating agreement (with original
score of 5-7). The total score of the four items on our
instrument represented a clinician's level of internal
work motivation. The total score ranges from 0 to 4;
a higher score indicated a higher level of motivation.
The Cronbach’s α value of the internal work
motivation questionnaire was 0.826, which indicated
that the scale had good internal consistency. The
Kaiser–Meyer–Olkin value of the questionnaire
was 0.705, indicating that the scale had good
structural validity. These results confirmed that the
questionnaire was an acceptable measurement tool.
Statistical analysis
STATA15.0 software (Stata Corporation; College
Station [TX], United States) was used to perform
descriptive and regression analyses of the collected
data. Logistic regression models with a significance
threshold of P<0.1 were used to analyse relationships
between internal work motivation and healthcare
quality.26 27 28 Two items, clinician workload × internal motivation interaction and financial incentive ×
internal motivation interaction, were added to the
model for analyses of heterogeneity. All regression
analyses were adjusted for fixed effects of disease
cases, standardised patients, and the coder.
Results
Characteristics of sample village clinicians
and clinics
In total, 225 village clinicians from 225 village clinics were included in this study. Table 1 describes the
basic characteristics of sample village clinicians.
The mean age of the clinicians was 49.20 years, and
196 clinicians (87.11%) were men. Among the 225
clinicians, 25 (11.11%) had attended college or above,
whereas seven (3.11%) had a practising clinician
qualification. Each clinician examined a mean of
171 patients per month. Mean salaries for village
clinicians were particularly low (slightly >1900 RMB
per month), and 103 clinicians (45.78%) had received
financial incentives.
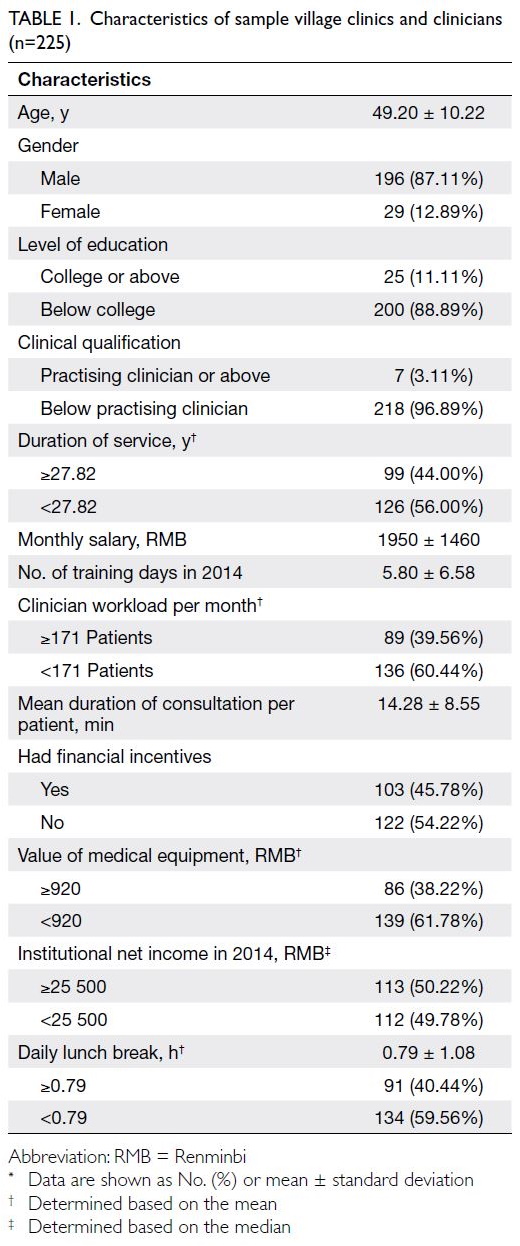
Table 1. Characteristics of sample village clinics and clinicians (n=225)
Table 1 also describes the characteristics of
sample village clinics. The mean value of medical
equipment was 920 RMB, and the mean institutional
net income in 2014 was 25 500 RMB. However, only
86 clinics (38.22%) had a medical equipment value
above the mean. This result indicates that the value of medical equipment considerably varied among
sample clinics, and the value of medical equipment
in most clinics was inadequate. Notably, clinics had
a mean lunch break length of <1 hour.
Healthcare quality among village clinicians
The unannounced standardised patients completed
225 disease cases (57, 87, and 81 cases of diarrhoea,
angina, and tuberculosis, respectively). Table 2
shows the healthcare quality among sample village
clinicians determined via three disease cases.
On average, the clinicians completed 17% of the
recommended consultation and examination items.
Furthermore, 129 clinicians (57.33%) completed
fewer than the mean number of recommended
consultation and examination items. Among all types
of cases, 73 clinicians (32.44%) provided a completely
or partially correct diagnosis. Furthermore, 94
clinicians (41.78%) provided correct or partly correct
treatments across all types of cases. Although the
results of these three indicators varied among
diseases, the percentages of clinicians with number
of recommended consultation and examination
items above the mean, number of correct diagnoses,
and number of treatments for each disease were
generally low.
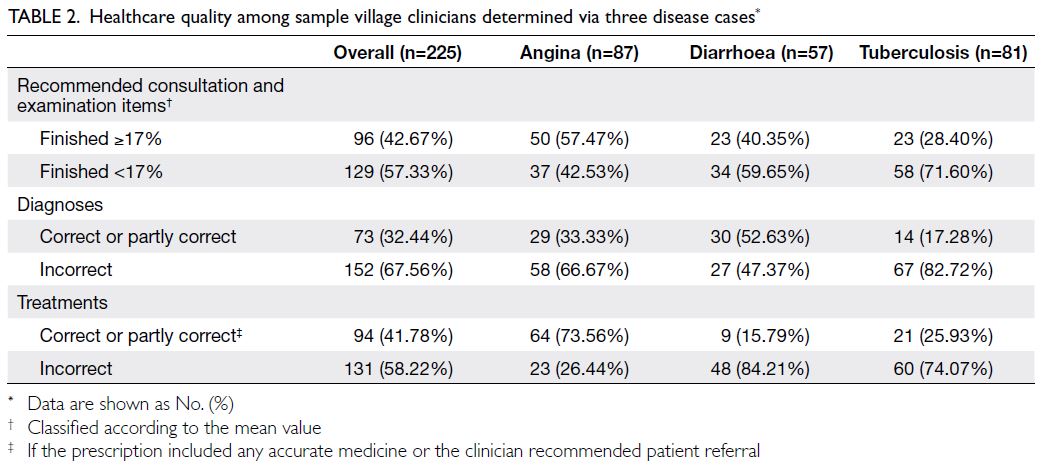
Table 2. Healthcare quality among sample village clinicians determined via three disease cases
Internal work motivation of village clinicians
Table 3 shows the levels of internal work motivation
among sample village clinicians. Overall, 213
clinicians (94.67%) believed that ‘I like what I do for
a living’ or ‘I enjoy my job’ motivated their work in
clinics. Furthermore, 187 (83.11%) and 206 (91.56%)
clinicians indicated that their respective main work
motivations were ‘because my job is interesting’ and
‘because my job is fun’. Integration of the scores for
the four items revealed that the mean overall score for
internal work motivation was 3.64 ± 0.85 (range, 0-4).
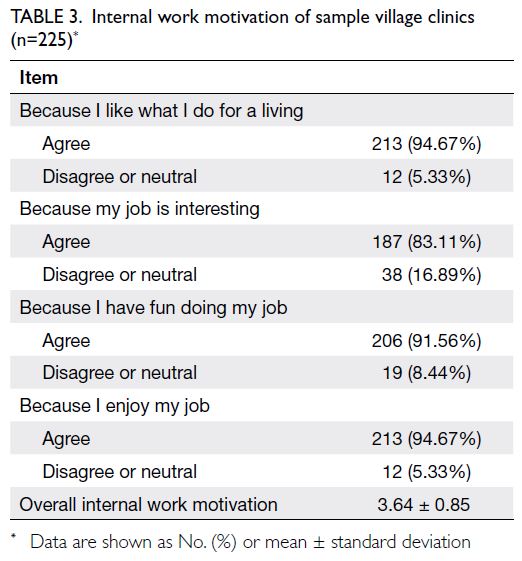
Table 3. Internal work motivation of sample village clinics (n=225)
Relationships between internal work
motivation and healthcare quality among village clinicians
Table 4 presents the results of logistic regression
analysis of the relationship between internal work
motivation and healthcare quality among village
clinicians. Internal work motivation had a positive
effect on clinical performance among sample clinicians. Specifically, for each one-unit increase
in internal work motivation, village clinicians were
42.17% (P<0.1) and 45.61% (P<0.1) more likely to
provide a correct or partially correct diagnosis and
treatment, respectively.
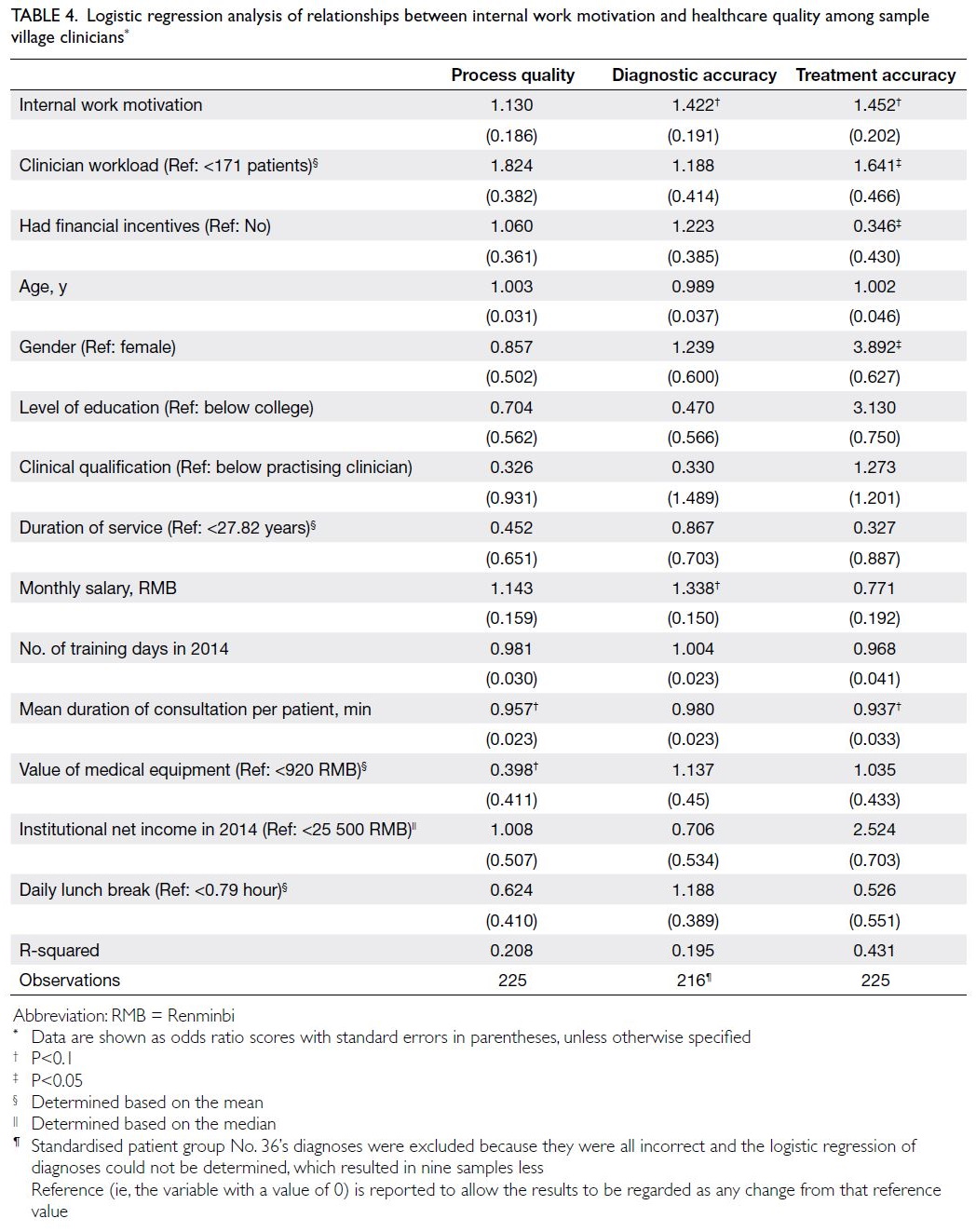
Table 4. Logistic regression analysis of relationships between internal work motivation and healthcare quality among sample village clinicians
Table 5 shows the results of heterogeneity
analysis from the perspective of clinician workload
and financial incentives. The clinician workload × internal motivation interaction was significantly
negatively correlated with diagnostic accuracy,
whereas the financial incentive × internal motivation
interaction was significantly positively correlated with treatment accuracy (P<0.1). These results
indicate that a heavier workload could hinder the
positive effect of internal motivation on diagnostic
accuracy among village clinicians. Furthermore, among village clinicians who received financial
incentives, the positive effect of their internal work
motivation on their treatments was stronger than
the corresponding effect among village clinicians
who did not receive financial incentives.
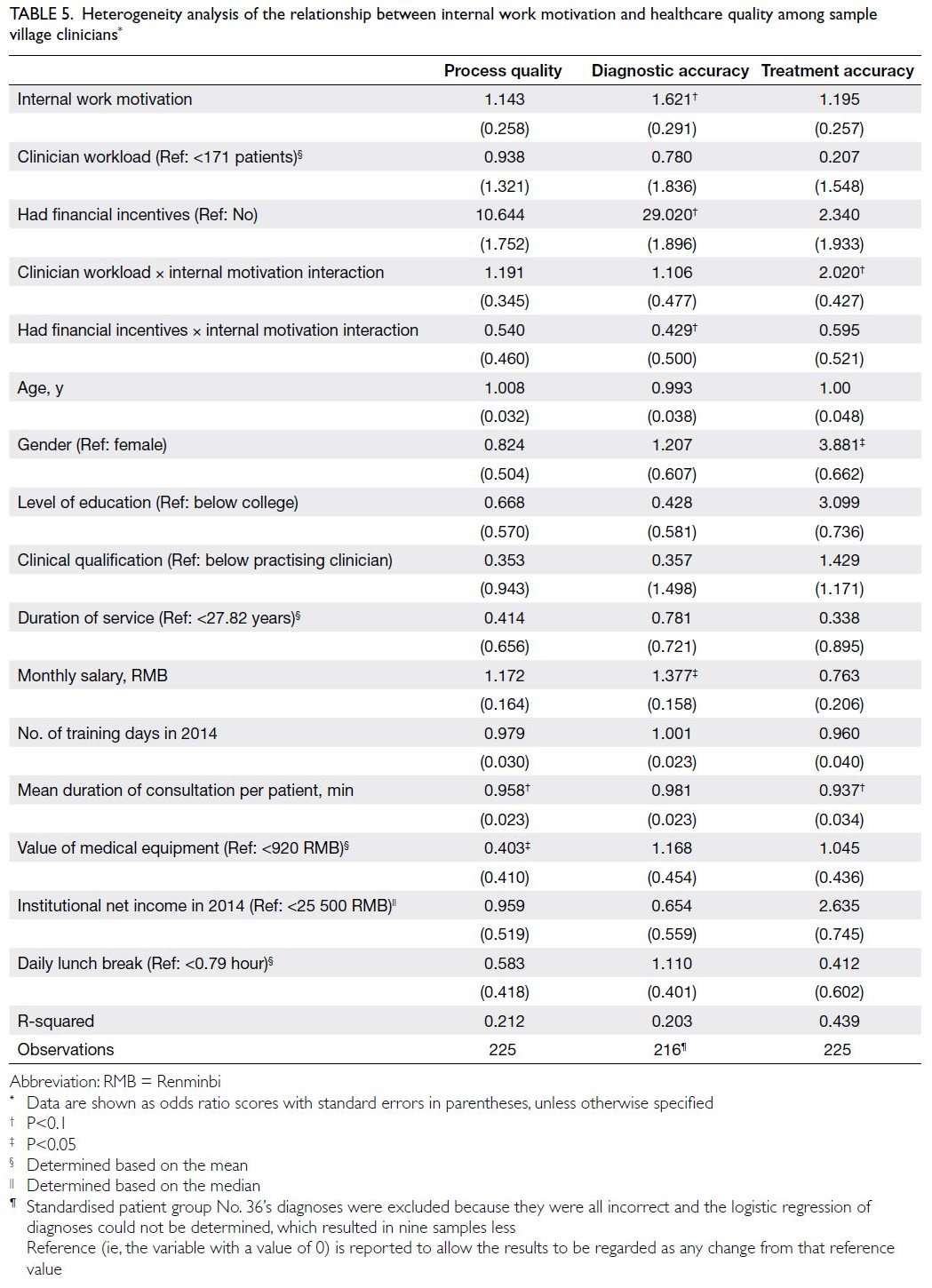
Table 5. Heterogeneity analysis of the relationship between internal work motivation and healthcare quality among sample village clinicians
Discussion
This study evaluated the healthcare quality among village clinicians in rural China and its relationship
with internal work motivation among these
clinicians, through an analysis of 225 rural village
clinicians from three provinces in 2015. There were
three main findings. First, healthcare quality among
village clinicians needed to be improved. Second,
village clinicians with stronger internal work
motivation were more likely to offer appropriate
treatment. Third, village clinicians with a lighter
workload (fewer patients per month) or financial
incentives exhibited a stronger positive correlation
between internal motivation and healthcare quality.
Generally, interactions between unannounced
standardised patients and sample village clinicians
showed that poor healthcare quality was provided
by village clinics in rural China. On average, village
clinicians completed only 17% of the recommended
consultation and examination items. The rates
of diagnostic accuracy and treatment accuracy
(including correct or partly correct treatment)
were 32.44% and 41.78%, respectively. Our findings
of poor healthcare quality are comparable with
the results of other studies performed at primary
health centres in rural China. For example, a study
based on the patient’s perspective, conducted in
Guangdong Province, highlighted the difficulty in
maintaining adequate coordination among primary
medical services.29 A survey using a standardised
patient method revealed that healthcare quality was
worse in rural China than in primary care settings
in Nairobi, Kenya.30 A systematic analysis of rural
township health centres in Shandong Province also
indicated a need for improved healthcare quality
among primary care clinicians.16
We found that internal work motivation was
generally high among village clinicians. The mean
internal work motivation score was 3.64 ± 0.85,
indicating that most village clinicians liked their jobs
and were interested in their careers. Consistent with
our findings, previous studies in other countries
showed that most medical workers had high levels
of internal work motivation.31 32 33 Although few
empirical studies have evaluated internal work
motivation among village clinicians, there is some
evidence that rural primary care clinicians in China
experience meaning and pleasure from engaging in
medical work.13 Additionally, similar to results in
other countries, we found that among the intrinsic
factors, most village clinicians believed that a love
for their career motivated them to work.33 34 35
Consistent with data from studies in other
countries,17 19 our empirical analysis demonstrated
significant positive correlations between internal
work motivation and healthcare quality among
village clinicians in rural China. According to affect
heuristic theory, this relationship presumably arises
because individuals rely on emotions to make
behavioural decisions, and a positive attitude will
lead to higher-quality behaviours.36 Empirical results
from other countries support this assumption.
A study in the United States demonstrated the
importance of internal work motivation in medical
behaviour decisions; clinicians with higher internal
motivation were more willing to maintain higher
quality in their work.17 The findings of studies in
developing countries, such as Ghana and Indonesia,
also indicated that work motivation can significantly
improve the quality of medical services provided
by clinicians.19 37 Thus, efforts to stimulate internal
work motivation among village clinicians may help
to improve their healthcare quality.
The results of heterogeneity analysis showed
that the positive effect of internal work motivation
on healthcare quality varied according to clinician
workload and financial incentives. Specifically,
internal work motivation had a stronger positive
effect on clinical performance among village
clinicians who had a lighter workload (fewer patients
per month). This is presumably because clinicians
with a heavier workload (more patients) are more
likely to experience burnout38 and a decreased
sense of autonomy,39 40 which could reduce internal
motivation and ultimately lead to a decline in work
performance.14 39 41 Additionally, compared with
village clinicians who did not receive financial
incentives, clinicians who received financial incentives
experienced a stronger positive effect on healthcare
quality because of their internal work motivation.
Studies of clinicians, combined with the results of
theoretical analyses in other fields (ie, motivational
synergy theory and self-decision theory), suggest
that the provision of financial incentives encourages
a belief of greater competence among clinicians; this
belief, in conjunction with internal work motivation,
enables clinicians to maintain high quality in their
work.13 14 41 42 Previous empirical studies have also demonstrated that performance-related financial
incentives can improve internal work motivation
among employees, leading to improvements in
performance.43
The results of these heterogeneity analyses
support efforts to enhance the positive effect of
internal work motivation on healthcare quality
by providing appropriate incentives for clinicians.
Consistent with this perspective, the Chinese
Government has been implementing incentive
programmes during the past decade to improve
healthcare quality among primary care clinicians in rural China.10 11 For example, the government is
actively restructuring the salary and performance
system, while asserting that healthcare systems at all
levels should engage in combined efforts to provide
additional financial incentives.44
To further promote internal work motivation
among clinicians and improve their work
performance, we recommend the revision of
governmental incentives policies, based on existing
policies. Specifically, medical institutions at all levels
should establish performance accountability45; and
emphasis should be placed on including physician
performance in assessments to incentivise high-quality
healthcare. Furthermore, medical institutions
at all levels should provide additional financial
incentives to clinicians based on assessments of
patient experiences. These programmes could
strengthen the positive effect of internal motivation
on work performance among clinicians and improve
their healthcare quality. Additionally, the workload
of primary clinicians should be carefully managed
to preserve the positive effect of their intrinsic
motivation on job performance.
This study had a few limitations. First, it was
a cross-sectional study, and the results represent
correlations rather than causal relationships.
Second, because we randomly selected samples from
Sichuan, Shaanxi, and Anhui provinces, our results
may not be fully representative of village clinicians
and village clinics throughout rural China. Third, the
reported level of internal work motivation may have
been overestimated because this variable was self-reported
by village clinicians.
Conclusion
Overall, healthcare quality was poor among village
clinicians in rural China. Furthermore, there
were positive correlations between internal work
motivation and healthcare quality among rural
village clinicians; these positive correlations were
stronger among clinicians with financial incentives
and lighter workload. Our findings suggest that the
Chinese Government should implement policies to
provide financial incentives for clinicians, with the
goal of enhancing internal work motivation among
village clinicians and improving their healthcare quality.
Author contributions
Concept or design: Q Gao, Y Shi, L Peng.
Acquisition of data: L Peng, S Song, Y Zhang.
Analysis or interpretation of data: L Peng, Q Gao, S Song.
Drafting of the manuscript: L Peng, Q Gao, Y Shi.
Critical revision of the manuscript for important intellectual content: All authors.
Acquisition of data: L Peng, S Song, Y Zhang.
Analysis or interpretation of data: L Peng, Q Gao, S Song.
Drafting of the manuscript: L Peng, Q Gao, Y Shi.
Critical revision of the manuscript for important intellectual content: All authors.
Conflicts of interest
As an International Editorial Advisory Board member of the journal, Y Shi was not involved in the peer review process.
Other authors have disclosed no conflicts of interest.
Acknowledgement
All authors thank the standardised patients and investigators for their contribution and hard work.
Funding/support
This work received funding from 111 Project (Grant No.: B16031), National Natural Science Foundation of China
(Grant No.: 72203134) and Innovation Capability Support
Program of Shaanxi, China (Grant No.: 2022KRM007).
Ethics approval
Ethical approval was obtained from the Institutional Review Board of Sichuan University, China (Protocol No.: K2015025). The board approved the verbal consent procedure. Participants
in this study were informed of the survey procedure and
consented to publication.
References
1. Babiarz KS, Miller G, Yi H, Zhang L, Rozelle S. China’s
new cooperative medical scheme improved finances of
township health centers but not the number of patients
served. Health Aff (Millwood) 2012;31:1065-74. Crossref
2. Shi Y, Xue H, Wang H, Sylvia S, Medina A, Rozelle S.
Measuring the quality of doctors’ health care in rural
China: an empirical research using standardized patients
[in Chinese]. Stud Labour Econ 2016;4:48-71.
3. Guo W, Sylvia S, Umble K, Chen Y, Zhang X, Yi H. The
competence of village clinicians in the diagnosis and
treatment of heart disease in rural China: a nationally
representative assessment. Lancet Reg Health West Pac
2020;2:100026. Crossref
4. Tan J, Yao Y, Wang Q. Comparative analysis of the
development and service utilisation of health resources
in Guangxi township hospitals and the whole country [in
Chinese]. Soft Sci Health 2019;33:46-50.
5. Sylvia S, Shi Y, Xue H, et al. Survey using incognito
standardized patients shows poor quality care in China’s
rural clinics. Health Policy Plan 2015;30:322-33. Crossref
6. Li X, Lu J, Hu S, et al. The primary health-care system in China. Lancet 2017;390:2584-94. Crossref
7. Yin X, Song F, Gong Y, et al. A systematic review of antibiotic utilization in China. J Antimicrob Chemother 2013;68:2445-52. Crossref
8. Virtual Health Library. Using indicators to measure
country pharmaceutical situations: fact book on WHO
level I and level II monitoring indicators. 2006. Available
from: https://pesquisa.bvsalud.org/portal/resource/pt/mis-19254. Accessed 30 Sep 2021.
9. Communist Party of China Central Committee, State
Council, People’s Republic of China. “Healthy China 2030”
Programme [in Chinese]. 2016. Available from: http://www.gov.cn/zhengce/2016-10/25/content_5124174.htm.
Accessed 30 Sep 2021.
10. State Council, People’s Republic of China. “Thirteenth
Five-Year” Sanitation and Health Plan [in Chinese]. 2017.
Available from: http://www.gov.cn/zhengce/content/2017-01/10/content_5158488.htm. Accessed 30 Sep 2021.
11. National Health and Family Planning Commission, National Development and Reform Commission, Ministry of Education of the People’s Republic of China, Ministry
of Finance of the People’s Republic of China, National
Administration of Traditional Chinese Medicine. National
Rural Doctor Education Plan (2011-2020) [in Chinese].
2013. Available from: http://www.gov.cn/gzdt/2013-10/30/content_2518099.htm. Accessed 20 Jan 2023.
12. State Council, People’s Republic of China. The 15th Meeting of the Standing Committee of the 13th National People’s Congress. Basic Medical Hygiene and Health Promotion
Law of the People’s Republic of China [in Chinese]. 2019.
Available from: http://www.gov.cn/xinwen/2019-12/29/content_5464861.htm. Accessed 5 Oct 2021.
13. Yuan B, Meng Q. Behaviour determinants of rural health workers: based on work motivation theory analysis [in Chinese]. Chin Health Econ 2012;31:50-2.
14. Kao AC. Driven to care: aligning external motivators with intrinsic motivation. Health Serv Res 2015;50 Suppl 2:2216-22. Crossref
15. Yuan B, Meng Q, Hou Z, Sun X, Song K. Analysis on incentive mechanism and motivation of rural health
providers [in Chinese]. Chin J Health Policy 2010;3:3-9.
16. Yuan S, Meng Q, Sun X. Studying on the quality of medical services in township health centres in view of
structural quality [in Chinese]. Chin Health Serv Manage
2012;29:841-4.
17. Green EP. Payment systems in the healthcare industry: an experimental study of physician incentives. J Econ Behav Organ 2014;106:367-78. Crossref
18. Mangkunegara AP, Agustine R. Effect of training, motivation and work environment on physicians’
performance. Acad J Interdiscip Stud 2016;5:173-88. Crossref
19. Al Aluf W, Sudarsih S, Musemedi DP, Supriyadi S. Assessing the impact of motivation, job satisfaction,
and work environment on the employee performance in
healthcare services. Int J Sci Technol Res 2017;6:337-41.
20. Hou X, Lu F. Effects of work values of millennial employees,
intrinsic motivation on job performance: the moderating
effect of organizational culture. Manage Rev 2018;30:157-68.
21. Li W, Mei J. Intrinsic motivation and employee performance: based on the effects of work engagement as
intermediary [in Chinese]. Manage Rev 2013;25:160-7.
22. Liao J, Jing Z, Liu W, Wang X. Promotion opportunity
stagnation and job performance: the mediating—role of
intrinsic motivation and perceived insider status. Ind Eng
Manage 2015;20:15-21.
23. Das J, Holla A, Das V, Mohanan M, Tabak D, Chan B. In
urban and rural India, a standardized patient study showed
low levels of provider training and huge quality gaps.
Health Aff (Millwood) 2012;31:2774-84. Crossref
24. Rethans JJ, Gorter S, Bokken L, Morrison L. Unannounced
standardised patients in real practice: a systematic
literature review. Med Educ 2007;41:537-49. Crossref
25. Amabile TM, Mueller J. Studying creativity, its processes,
and its antecedents: an exploration of the componential
theory of creativity. In: Zhou J, Shalley CE, editors.
Handbook of Organizational Creativity. New York:
Lawrence Erlbaum Associates; 2008: 33-64.
26. Lee KI, Koval JJ. Determination of the best significance
level in forward step-wise logistic regression. Commun
Stat Simul Comput 1997;2:559-75. Crossref
27. Maneejuk P, Yamaka W. Significance test for linear
regression: how to test without P-values? J Appl Stat 2020;31:827-45. Crossref
28. Feise R. Do multiple outcome measures require p-value adjustment? BMC Med Res Methodol 2002;17:1471-2288-2-8. Crossref
29. Feng S. Analysis of the quality of primary care and the
influencing factors in rural Guangdong Province—based
on demander perspective [in Chinese]. Chin Health Serv Manage 2016;33:824-7.
30. Daniels B, Dolinger A, Bedoya G, et al. Use of standardised patients to assess quality of healthcare in Nairobi, Kenya: a pilot, cross-sectional study with international comparisons. BMJ Glob Health 2017;2:e000333.
31. Settineri S, Merlo EM, Frisone F, et al. The experience of health and suffering in the medical profession. Mediterr J Clin Psychol 2018;6:1-14.
32. Toode K, Routasalo P, Helminen M, Suominen T. Hospital
nurses’ individual priorities, internal psychological states
and work motivation. Int Nurs Rev 2014;61:361-70. Crossref
33. Tsounis A, Sarafis P, Bamidis PD. Motivation among
physicians in Greek public health-care sector. Br J Med
Med Res 2014;4:1094-105. Crossref
34. Ferraro T, dos Santos NR, Moreira JM, Pais L. Decent
work, work motivation, work engagement and burnout in
physicians. Int J Appl Posit Psychol 2020;5:13-35. Crossref
35. Lochner L, Wieser H, Mischo-Kelling M. A qualitative
study of the intrinsic motivation of physicians and other
health professionals to teach. Int J Med Educ 2012;3:209-15. Crossref
36. Slovic P, Finucane ML, Peters E, MacGregor DG. The affect heuristic. Eur J Oper Res 2007;177:1333-52. Crossref
37. Alhassan RK, Spieker N, van Ostenberg P, Ogink A,
Nketiah-Amponsah E, de Wit TF. Association between
health worker motivation and healthcare quality efforts in
Ghana. Hum Resour Health 2013;11:37. Crossref
38. Ward ZD, Morgan ZJ, Peterson LE. Family physician burnout does not differ with rurality. J Rural Health
2021;37:755-61. Crossref
39. Wang Y, Hu XJ, Wang HH, et al. Follow-up care delivery in community-based hypertension and type 2 diabetes management: a multi-centre, survey study among rural primary care physicians in China. BMC Fam Pract 2021;22:224. Crossref
40. Shirom A, Nirel N, Vinokur AD. Work hours and caseload as predictors of physician burnout: the mediating effects by perceived workload and by autonomy. Appl Psychol 2010;59:539-65. Crossref
41. Deci EL, Ryan RM. Intrinsic Motivation and Self-Determination in Human Behavior. New York: Springer;
1985. Crossref
42. Amabile TM. Motivational synergy: toward new conceptualizations of intrinsic and extrinsic motivation in
the workplace. Hum Resour Manage Rev 1993;3:185-201. Crossref
43. Eisenberger R, Aselage J. Incremental effects of reward on experienced performance pressure: positive outcomes for intrinsic interest and creativity. J Organiz Behav
2009;30:95-117. Crossref
44. Qin J, Li S, Lin C. Reform progress and development strategy of incentive mechanism for training and use of
general practitioners in China [in Chinese]. Chin Gen
Pract 2020;23:2351-8.
45. Li X, Krumholz HM, Yip W, et al. Quality of primary health care in China: challenges and recommendations. Lancet 2020;395:1802-12. Crossref