Hong Kong Med J 2022 Apr;28(2):182.e1–2
Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Transmural perforation by fish bone from
stomach to liver
X Liu, MD1; J Shi, MD2
1 Department of Radiology, Hospital of Chengdu University of Traditional
Chinese Medicine, Chengdu, China
2 Department of Nursing, Hospital of Chengdu University of Traditional
Chinese Medicine, Chengdu, China
Corresponding author: Ms J Shi (267126966@qq.com)
 Full paper in PDF
Full paper in PDF
A 46-year-old man was admitted to the emergency
department with a 3-day history of epigastric
abdominal pain associated with nausea. His
temperature was 36.5°C, pulse 74 beats per minute
and blood pressure 135/70 mm Hg. Physical
examination revealed mild epigastric tenderness and
rebound tenderness in the upper abdomen. Basic
laboratory test results were normal. Abdominal
computed tomography (CT) scan (Fig) revealed a
radiodense linear foreign body measuring 3 cm,
extending transmurally through the lesser curvature
of the stomach and penetrating the liver capsule.
Inflamed tissue surrounding the pylorus was also noted. Pneumoperitoneum was evident as free gas
under the diaphragm. The patient was kept nil by
mouth and transferred for emergency laparoscopy.
An oesophagogastroduodenoscopy was performed
and a fish bone penetrating the stomach wall was
found. Clipping was performed after fish bone
removal. Empiric intravenous antibiotic (tazobactam
4 g/8 h) was prescribed before and after the
oesophagogastroduodenoscopy. The patient made
an uneventful recovery and was discharged home
6 days after surgery.
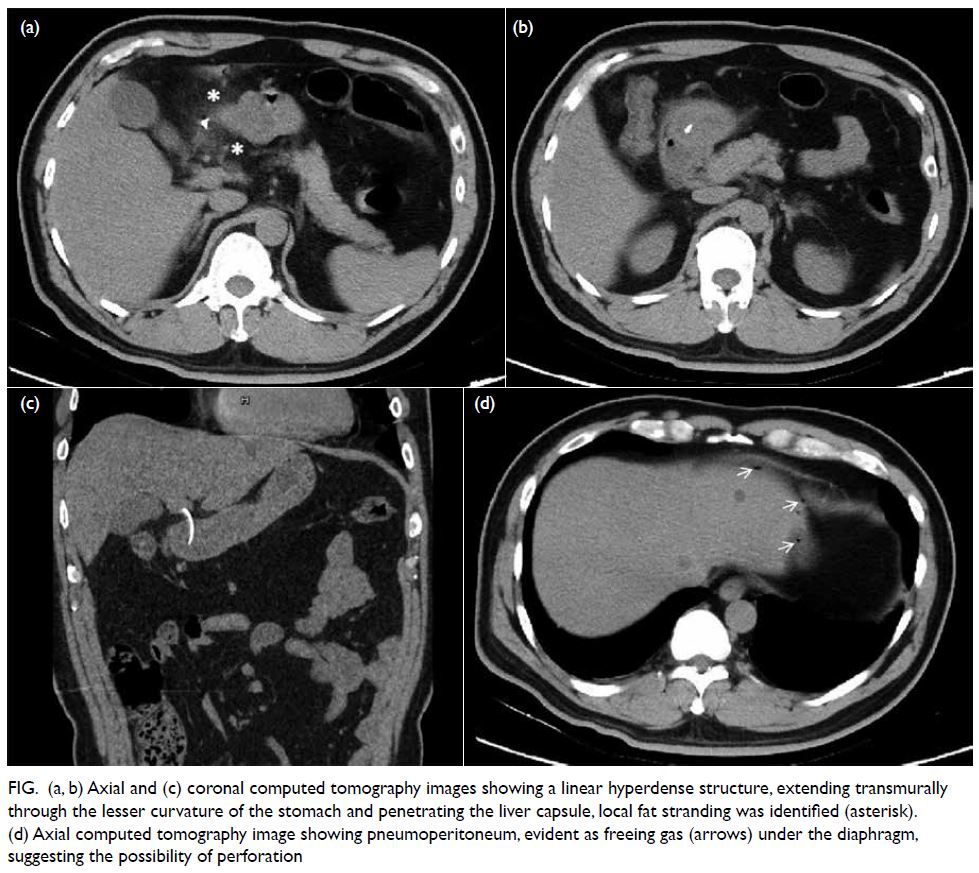
Figure. (a, b) Axial and (c) coronal computed tomography images showing a linear hyperdense structure, extending transmurally through the lesser curvature of the stomach and penetrating the liver capsule, local fat stranding was identified (asterisk). (d) Axial computed tomography image showing pneumoperitoneum, evident as freeing gas (arrows) under the diaphragm, suggesting the possibility of perforation
After ingestion, most fish bones pass through
the gastrointestinal tract within a week and cause no serious complications. Gastrointestinal perforation
by fish bone is a rare medical emergency. Clinical
symptoms are often atypical and may vary from mild
to severe depending on the site of perforation and
the degree of inflammation.1 In addition to a non-specific
clinical presentation, a history of foreign
body ingestion is rarely available. The patient in
this report was unaware of fish bone ingestion.
Laboratory findings are also non-specific and usually
demonstrate elevated inflammatory markers. Thus, a
diagnosis of fish bone perforation can be challenging
and is often delayed. The radiologist plays an essential
role in the detection of fish bone perforation and
associated complications.
Computed tomography is considered the
most effective means by which to identify foreign
bodies and their associated complications due to
its high resolution and high-quality multiplanar
capabilities.2 The main imaging features of fish bone
perforation on CT scan are a linear hyperdense
structure in the gastrointestinal tract, inflammatory
changes surrounding the perforation site, and
pneumoperitoneum.2 3 Pneumoperitoneum is
a rare yet important finding that can signal the
possibility of perforation. In our case, multiplanar
CT reconstructions revealed that the fish bone
had partially perforated the stomach wall into
the adjacent hepatic parenchyma, causing
perigastric inflammatory changes. In addition,
pneumoperitoneum was identified under the
diaphragm. This report provides a reference for
clinicians. Early endoscopic or surgical removal of a
foreign body from the stomach causing complications
is recommended.
Author contributions
Concept or design: X Liu.
Acquisition of data: All authors.
Analysis or interpretation of data: All authors.
Drafting of the manuscript: All authors.
Critical revision of the manuscript for important intellectual content: All authors.
Acquisition of data: All authors.
Analysis or interpretation of data: All authors.
Drafting of the manuscript: All authors.
Critical revision of the manuscript for important intellectual content: All authors.
All authors had full access to the data, contributed to the
study, approved the final version for publication, and take
responsibility for its accuracy and integrity.
Conflicts of interest
The authors declared no potential conflicts of interest.
Funding/support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This study was approved by the Hospital of Chengdu
University of Traditional Chinese Medicine Research Ethics
Committee (Ref: 2021524). Informed consent was obtained
from the patient.
References
1. Yi L, Cheng Z, Zhou Y, et al. Fishbone foreign body
ingestion in duodenal papilla: a cause of abdominal pain
resembling gastric ulcer. BMC Gastroenterol 2020;20:323. Crossref
2. Paixão TS, Leão RV, de Souza Maciel Rocha Horvat N, et al.
Abdominal manifestations of fishbone perforation: a
pictorial essay. Abdom Radiol (NY) 2017;42:1087-95. Crossref
3. Davarpanah AH, Eberhardt LW. Case 282: fishbone pylephlebitis. Radiology 2020;297:239-43. Crossref