Hong Kong Med J 2021 Dec;27(6):457.e1–2
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Emphysematous cystitis complicated by liver abscess
L Zeng, MD1; Q Wang, MD2
1 Department of Radiology, Hospital of Chengdu University of Traditional Chinese Medicine, Sichuan, China
2 Department of Ultrasound, Hospital of Chengdu University of Traditional Chinese Medicine, Sichuan, China
Corresponding author: Dr Q Wang (444028177@qq.com)
 Full paper in PDF
Full paper in PDF
In July 2019, a 54-year-old woman with type 2
diabetes mellitus and suboptimal drug compliance
with metformin and gliclazide presented to the
emergency department complaining of abdominal
pain, progressive weakness, and confusion. Her body
temperature was 39.1°C and blood tests revealed
serum glucose 29.1 mmol/L; haemoglobin A1c 10.4%;
serum glucose 29.1 mmol/L; haemoglobin A1c 10.4%;
C-reactive protein 224.3 mg/L; and white cell count
11.9 × 109/L with 92.8% segmented neutrophils;
and serum creatinine 437.4 mmol/L. Computed
tomography scan of the abdomen and pelvis without
contrast revealed a cystic gas-producing liver lesion
and diffuse intramural gas dissecting the urinary
bladder wall with extension to the left kidney (Fig). A
diagnosis was made of acute emphysematous cystitis
complicated by liver abscess.
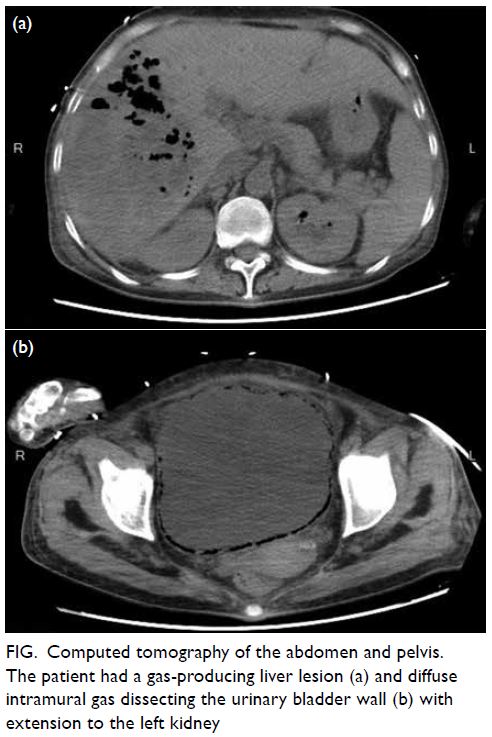
Figure. Computed tomography of the abdomen and pelvis. The patient had a gas-producing liver lesion (a) and diffuse intramural gas dissecting the urinary bladder wall (b) with extension to the left kidney
Percutaneous drainage of the liver abscess was
performed under ultrasound guidance. Klebsiella
pneumoniae, sensitive to meropenem, was cultured from the urine and drained pus. The patient was
transferred to the intensive care unit and treated
with resuscitation, glycaemic control, and broad-spectrum
antibiotics with intravenous meropenem.
Meropenem was continued for the initial 7 days
and then changed to ceftazidime plus amikacin
according to susceptibility testing results. Her
symptoms subsided and blood parameters improved
gradually. She made an uneventful recovery and was
discharged from the hospital on day 20.
Emphysematous cystitis is an uncommon type
of infection characterised by gas collections within
the bladder wall and lumen. It is usually caused by
gas-producing pathogens such as Escherichia coli
and Klebsiella pneumoniae.1 Predisposing factors
are diabetes, female sex, obstructive uropathy and
possibly immunosuppression. Gas is believed to be
produced by fermentation of albumin or glucose by
the infecting organisms. Emphysematous cystitis
combined with liver abscess is rare. The mechanisms
of emphysematous cystitis are not well understood.
Some reports emphasise that pathogenesis may be
related to hematogenous transmission from the liver
abscess.2 3 Immunosuppression related to poorly
controlled diabetes is another contributing factor.
Clinical presentation of emphysematous
cystitis varies. Our patient presented with systemic
manifestations of septic shock and severe upper
abdominal pain secondary to the liver abscess.
She reported no lower urinary tract symptoms.
Computed tomography is the best diagnostic
modality with its high sensitivity when assessing
the extent of gas patterns. Appropriate antibiotic
therapy, correction of the underlying disorder, and
adequate drainage is the recommended treatment.
Author contributions
Concept or design: Both authors.
Acquisition of data: L Zeng.
Analysis or interpretation of data: L Zeng.
Drafting of the manuscript: L Zeng.
Critical revision of the manuscript for important intellectual content: Q Wang.
Acquisition of data: L Zeng.
Analysis or interpretation of data: L Zeng.
Drafting of the manuscript: L Zeng.
Critical revision of the manuscript for important intellectual content: Q Wang.
Both authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Conflicts of interest
The authors declared no potential conflicts of interest.
Funding/support
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This study was approved by the Hospital of Chengdu
University of Traditional Chinese Medicine Research Ethics
Committee. Informed consent was obtained from the patient.
References
1. Amano M, Shimizu T. Emphysematous cystitis: a review of the literature. Intern Med 2014;53:79-82. Crossref
2. Lai CC. Concomitant emphysematous cystitis and liver abscess. Korean J Intern Med 2018;33:839-40. Crossref
3. Su YC, Chen CC. Emphysematous cystitis complicating Klebsiella pneumoniae liver abscess. Am J Emerg Med
2006,24:256-7.Crossref