© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE CME
Total knee arthroplasty is safe for patients aged ≥80 years in Hong Kong
Amy Cheung, FHKCOS, FHKAM (Orthopaedic Surgery)1; PK Chan, FHKCOS, FHKAM (Orthopaedic Surgery)1; Henry Fu, FHKCOS, FHKAM (Orthopaedic Surgery)1; MH Cheung, FHKCOS, FHKAM (Orthopaedic Surgery)2; Vincent WK Chan, FHKCOS, FHKAM (Orthopaedic Surgery)1; CH Yan, FHKCOS, FHKAM (Orthopaedic Surgery)2; KY Chiu, FHKCOS, FHKAM (Orthopaedic Surgery)2
1 Department of Orthopaedics and Traumatology, Queen Mary Hospital, Hong Kong
2 Department of Orthopaedics and Traumatology, The University of Hong Kong, Hong Kong
Corresponding author: Dr Amy Cheung (amyylcheung@ortho.hku.hk)
 Full paper in PDF
Full paper in PDF
Abstract
Introduction: Total knee arthroplasty (TKA) is
an efficacious operation that improves pain and
function in patients with knee arthritis. Because of
the population ageing trend in Hong Kong, there is a
need to determine the safety profile of TKA in older
patients. This study examined the age of patients
who underwent TKA in the past 10 years in Hong
Kong; the aim was to investigate the mortality safety
profile and clinical outcomes of TKA in patients
aged ≥80 years.
Methods: This study included all patients who
underwent primary TKA in the Hospital Authority
(HA) from 2010 to 2019. Incidences of 30-day,
90-day, and 1-year mortality were established.
Clinical outcomes of patients aged ≥80 years in one
cluster of HA hospitals were assessed.
Results: Between 2010 and 2019, 25 040 TKA
procedures were conducted in all HA hospitals;
2491 were conducted in patients aged ≥80 years.
The median age at operation was higher during
2015-2019 than during 2010-2014 (70 vs 69 years;
P<0.001); furthermore, an increase was observed
in the proportion of patients aged ≥80 years at the time of operation. Incidences of 30-day, 90-day, and
1-year mortality were 0.156%, 0.35%, and 1.09%, respectively.
Conclusions: In this first study to examine the safety
profile of TKA in older patients in Hong Kong, the
mean age at the time of TKA and proportion of
patients aged ≥80 years have steadily risen in the past
decade. Even in older patients, TKA is a reasonably
safe procedure.
New knowledge added by this study
- The total knee arthroplasty (TKA) caseload, mean age of patients, and proportion of patients aged ≥80 years at the time of TKA in Hong Kong has risen steadily in the past 10 years.
- The overall mortality rate within 1 year after surgery among patients aged ≥80 years at the time of TKA was 1.09%, which is substantially lower than overall mortality rate of the older general population in Hong Kong.
- TKA is a reasonably safe and efficacious procedure, even in patients aged ≥80 years at the time of operation.
- Adequate resources should be allocated towards TKA in the near future to meet the increasing needs of the ageing population.
- When adequate perioperative assessment and management are instituted, older patients should not be advised to avoid TKA for the management of end-stage knee arthritis.
Introduction
It has been projected that, by year 2036, one in three
people in Hong Kong will be aged ≥65 years.1 Because
the life expectancy of the Hong Kong population
consistently ranks among the highest worldwide,
the medical and social needs of older individuals are
expected to increase rapidly in the next few decades.
The waiting time for joint arthroplasty in Hong
Kong’s Hospital Authority (HA) system increased
from 33 months in 20102 to 50 months in 20193,
reflecting increasing demand for such procedures in
our population.
Total knee arthroplasty (TKA) is a highly
successful operation that provides substantial pain
relief and functional improvement for patients with
end-stage knee arthritis.4 However, in Hong Kong,
there is the prevalent belief among many members of
the community that older patients, particularly those
aged ≥80 years, have a substantial risk of mortality
after TKA. Therefore, despite substantial pain and
debilitation, older patients have often avoided TKA
as treatment for their knee arthritis. However, this
avoidance may no longer be a reasonable approach
in the era of modern arthroplasty.
This study examined the age of patients who
underwent TKA in the past 10 years in Hong Kong.
The aim of the study was to determine the mortality
safety profile and clinical outcomes after TKA in
patients aged ≥80 years at the time of operation.
Methods
All patients who underwent primary TKA between 2010 and 2019 in public hospitals operated by the
HA were included in the study. Patient data were
extracted from the HA Clinical Data Analyses
and Reporting System. Baseline demographic
characteristics (eg, age, sex, and diagnosis at the time
of operation) were recorded. Patients were stratified
according to age (<80 or ≥80 years) at the time of
the operation. Incidences of 30-day, 90-day, and
1-year mortality after TKA, as well as the incidence
of emergency readmission within 28 days after TKA,
were calculated.
Furthermore, all patients who had undergone
TKA between 2010 and 2019 in the HA’s Hong Kong
West Cluster of hospitals, who were aged ≥80 years
at the time of operation, were identified for inclusion
in the study. The Hong Kong West Cluster comprises
seven hospitals, providing a total of 3142 beds.3
Baseline preoperative parameters, including
the Charlson Comorbidity Index (CCI),5 as well
as the Knee Society Knee Score (KSKS) and Knee
Society Knee Functional Assessment (KSFA)
scores,6 7 were recorded. Rehabilitation outcomes,
including KSKS and KSFA scores, were recorded at
1 year after surgery and at the latest follow-up.
For data collection and statistical analyses, SPSS (Windows version 26) was used. Age, CCI
score, KSKS, and KSFA score were all non-normally
distributed, according to the Kolmogorov–Smirnov
test. Therefore, the Mann-Whitney U test was used
to compare the median ages of patients during 2010-2014 and 2015-2019; to compare the median CCI
score between older patients who died within 1 year
of the operation and patients who survived; and to
compare KSKS and KSFA scores before surgery and
at 1 year after surgery.
Results
Demographics of patients undergoing total
knee arthroplasty in Hong Kong between 2010 and 2019
Between 2010 and 2019, 25 040 TKA procedures
were conducted in all HA hospitals. During the
same period, 3835 TKA procedures were conducted
in the authors’ hospital cluster. An increasing trend
was observed in the number of TKA procedures
each year; the yearly caseload in 2019 was more than
double the yearly caseload in 2010 (Table, Fig).
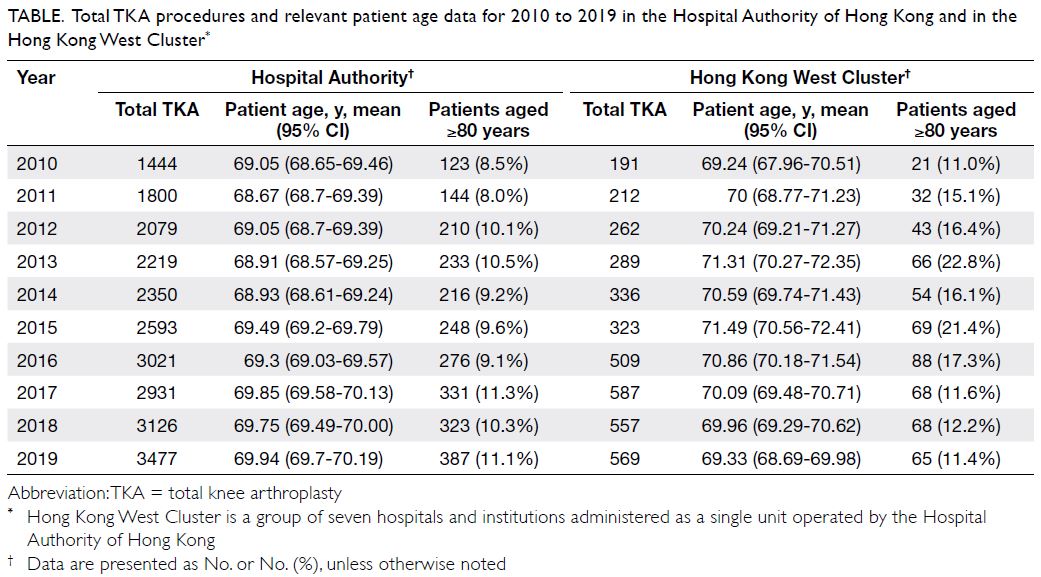
Table. Total TKA procedures and relevant patient age data for 2010 to 2019 in the Hospital Authority of Hong Kong and in the Hong Kong West Cluster
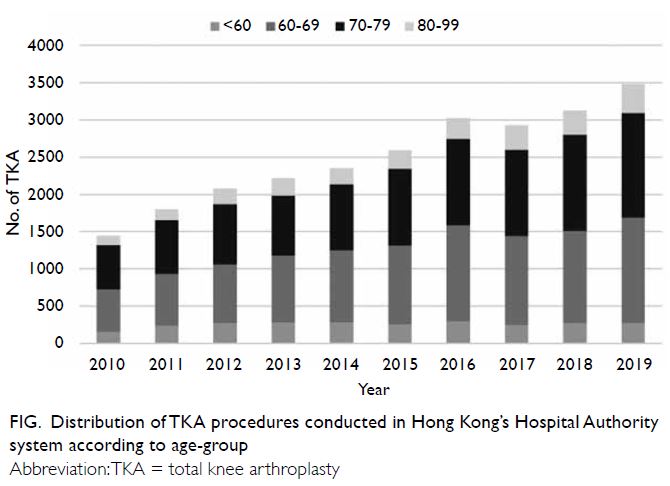
Figure. Distribution of TKA procedures conducted in Hong Kong’s Hospital Authority system according to age-group
For all HA hospitals, the mean age (± standard deviation) at the time of operation throughout the study period was 69.4 ± 7.7 years (range, 18-94).
Median age at the time of operation significantly
increased from 69 years (interquartile range [IQR],
58-80) in 2010-2014 to 70 years (IQR, 59-81) in
2015-2019 (P<0.001).
An increase in the proportion of patients aged ≥80 years at the time of operation was observed
throughout the study period (Table, Fig).
Safety of total knee arthroplasty in patients aged ≥80 years
Between 2010 and 2019, 2491 TKA procedures
were conducted in all HA hospitals in patients aged
≥80 years. The median age at operation was 82 years
(IQR, 80-84). Mortality rates within 30 and 90 days
after surgery were 0.156% and 0.35%, respectively.
The mortality rate within 1 year after surgery was
1.09%. In total, 5.3% of patients required emergency
readmission within 28 days of TKA.
During the study period, 22 549 TKA
procedures were conducted in all HA hospitals in
patients aged <80 years. The mean age (± standard
deviation) at operation was 67.9 ± 6.8 years (range,
14-79). Mortality rates at 30 days, 90 days, and
1 year after surgery were 0.047%, 0.128%, and 0.441%,
respectively. In total, 4.02% of patients required
emergency readmission within 28 days after surgery.
Between 2010 and 2019, 574 TKA procedures were conducted in patients aged ≥80 years at the
time of operation in the authors’ HA hospital cluster.
The mean age (± standard deviation) at operation
was 82.9 ± 2.6 years (range, 80-93).
The mean CCI score (± standard deviation) at
the time of operation was 4 ± 1.1 (range, 4-11). The
CCI score was not significantly different between
older patients who died within 1 year after surgery
and older patients who survived beyond this time
period (median: 5 vs 4; P=0.565).
Clinical outcomes in older patients after total knee arthroplasty
The median KSKS improved from 45 before surgery to 94 at 1 year after surgery (P<0.001). The median KSFA scores improved from 45 before surgery to 55
at 1 year after surgery (P<0.001).
Discussion
In the past decade in Hong Kong, the proportion
of patients aged ≥80 years at the time of operation
increased from 8.5% in 2010 to 11.1% in 2019.
Moreover, the proportions of patients aged ≥80 years
at the time of operation were 9.3% and 10.3% during
2010-2014 and 2015-2019, respectively. These
proportions are higher than the values reported by
Yan et al,8 who examined the demographics of TKA
usage in the preceding decade (ie, 2000-2009) in
Hong Kong.
In 2019 in Hong Kong, the mean age at the
time of operation was 69.9 years; this was similar to
the mean ages from studies in the United Kingdom
(69 years)9 and Australia (68.5 years)10. Furthermore,
the mean age at the time of the operation increased
throughout the study period among all patients
undergoing TKA in the HA system. This pattern has
also been observed in Taiwan,11 but it contrasts with
the findings in the United States and Canada, where
overall decreases in mean age have been observed.12
Overall, the mortality rates among older
patients in the present study were similar to those
reported in other countries.13 14 However, the
mortality rates among older patients undergoing
TKA in the present study are higher than the
mortality rates reported among patients of all ages
undergoing TKA in the HA15 (0.1%, 0.2% and 0.7%
at 30 days, 90 days and 1 year, respectively) and in
other localities (0.18% within 30 days after surgery).16 Although the mean age of the overall patient cohort
was not reported in the study by Lee et al,15 the mean
ages of the mortality and non-mortality groups
were 78 and 64 years, respectively. These are both
substantially lower than the mean age at operation
for the older patient group in the present study
(82.8 years). Although mortality rates at 30 days,
90 days, 1 year and 5 years after surgery differed
between the present study and the study by Lee et al,15
the values were generally comparable.
The differences in mortality risk between
older and younger patients in the present study are
consistent with the findings in a meta-analysis by
Kuperman et al,17 who reported increased mortality
in older patients after TKA. This is likely related
to underlying differences in the inherent mortality
risks between older and younger patients caused
by age-related increases in the number of medical
co-morbidities. In Hong Kong in 2018, the age-specific
mortality rates for the general population
aged 80 to 84 years were 5.5% and 3.2% for men
and women, respectively.18 In the present study, the
overall mortality rate within 1 year after surgery for
the older patient cohort was 1.09%, substantially
lower than the overall mortality rate of the older
general population in Hong Kong. This likely reflects
the stringent preoperative screening protocol used
for older TKA candidates, which is intended to
minimise the risk of mortality.13 15 Therefore, with
careful perioperative assessment and management,
mortality risk after TKA can be minimised, even in
older patients.
Finally, the present study revealed that
both KSKS and KSFA scores were significantly
improved at 1 year after TKA, compared with scores
before surgery. Therefore, pain, objective physical
examination findings, and function in terms of
walking and ability to climb stairs can be significantly
improved after TKA, even in older patients. Our
results support the findings in previous literature.19 20
An important limitation of the retrospective
study design was that it did not allow us to control
for confounding variables, such as differences in
surgical expertise and standards of perioperative care
among the centres included in this study. However,
to our knowledge, this is the only study regarding
the incidence of mortality after TKA among older
patients in Hong Kong. The results of this study are
important for our locality because they describe
TKA outcomes from all HA hospitals in the past
10 years in a large cohort of patients.
In conclusion, this study showed that the mean age at the time of TKA has steadily risen in the past
10 years, consistent with population ageing trends
in Hong Kong. Furthermore, the findings indicate
that TKA is a safe and efficacious procedure, even
in older patients. Therefore, provided that proper
perioperative assessment and management are conducted, advanced age should not be a deterrent
for TKA in the management of end-stage knee
arthritis among older patients who can substantially
benefit from this procedure.
Author contributions
Concept or design: A Cheung, CH Yan, KY Chiu.
Acquisition of data: A Cheung, PK Chan, H Fu, VWK Chan, MH Cheung.
Analysis or interpretation of data: A Cheung, PK Chan, H Fu, VWK Chan, MH Cheung.
Drafting of the manuscript: A Cheung, PK Chan, KY Chiu.
Critical revision of the manuscript for important intellectual content: A Cheung, CH Yan, KY Chiu.
Acquisition of data: A Cheung, PK Chan, H Fu, VWK Chan, MH Cheung.
Analysis or interpretation of data: A Cheung, PK Chan, H Fu, VWK Chan, MH Cheung.
Drafting of the manuscript: A Cheung, PK Chan, KY Chiu.
Critical revision of the manuscript for important intellectual content: A Cheung, CH Yan, KY Chiu.
All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Conflicts of interest
All authors have disclosed no conflicts of interest.
Funding/support
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This research has received approval from the Institutional Review Board of The University of Hong Kong/Hospital Authority Hong Kong West Cluster (Ref UW 20-161).
References
1. Census and Statistics Department, Hong Kong SAR Government. Hong Kong population projections for 2017
to 2066. Available from: https://www.censtatd.gov.hk/
media_workers_corner/pc_rm/hkpp2017_2066/index.jsp.
Accessed 19 Mar 2020.
2. Bureau Food and Health Bureau. Legislative Council Panel
on Health Services Improvement on Joint Replacement
Surgeries in the Hospital Authority. 2011. Available from:
https://www.legco.gov.hk/yr10-11/english/panels/hs/papers/hs0613cb2-1992-3-e.pdf. Accessed 20 Mar 2020.
3. Hospital Authority website. Available from: https://www.ha.org.hk/visitor/ha_visitor_text_index.asp?Content_ID=221223&Lang=ENG&Dimension=100. Accessed on 24
Sep 2021.
4. Pavone V, Boettner F, Fickert S, Sculco TP. Total condylar knee arthroplasty: a long-term followup. Clin Orthop Relat Res 2001(388):18-25. Crossref
5. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in
longitudinal studies: development and validation. J Chronic
Dis 1987;40:373-83. Crossref
6. Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res 1989;(248):13-4. Crossref
7. Lingard EA, Katz JN, Wright RJ, Wright EA, Sledge CB, Kinemax Outcomes Group. Validity and responsiveness of the Knee Society Clinical Rating System in comparison
with the SF-36 and WOMAC. J Bone Joint Surg Am
2001;83:1856-64. Crossref
8. Yan CH, Chiu KY, Ng FY. Total knee arthroplasty for primary knee osteoarthritis: changing pattern over the past 10 years. Hong Kong Med J 2011;17:20-5.
9. National Joint Registry. National Joint Registry 16th Annual Report 2019. Available from: https://reports.njrcentre.org.uk/portals/0/pdfdownloads/njr%2016th%20annual%20report%202019.pdf. Accessed 4 Mar 2020.
10. Australian Orthopaedic Association National Joint
Replacement Registry (AOANJRR). Hip, Knee & Shoulder
Arthroplasty: 2020 Annual Report. Adelaide: AOA; 2020:
1-474. Available from: https://aoanjrr.sahmri.com/annual-reports-2020. Accessed 21 Sep 2021.
11. Lin FH, Chen HC, Lin C, et al. The increase in total knee
replacement surgery in Taiwan: a 15-year retrospective
study. Medicine (Baltimore) 2018;97:e11749. Crossref
12. Ravi B, Croxford R, Reichmann WM, Losina E, Katz JN,
Hawker GA. The changing demographics of total joint
arthroplasty recipients in the United States and Ontario
from 2001 to 2007. Best Pract Res Clin Rheumatol
2012;26:637-47. Crossref
13. Hunt LP, Ben-Shlomo Y, Clark EM, et al. 45-Day mortality
after 467,779 knee replacements for osteoarthritis from
the National Joint Registry for England and Wales: an
observational study. Lancet 2014;384:1429-36. Crossref
14. Clement ND, MacDonald D, Howie CR, Biant LC. The
outcome of primary total hip and knee arthroplasty in patients aged 80 years or more. J Bone Joint Surg Br
2011;93:1265-70. Crossref
15. Lee QJ, Mak WP, Wong YC. Mortality following primary
total knee replacement in public hospitals in Hong Kong.
Hong Kong Med J 2016;22:237-41. Crossref
16. Belmont PJ Jr, Goodman GP, Waterman BR, Bader JO,
Schoenfeld AJ. Thirty-day postoperative complications and
mortality following total knee arthroplasty: incidence and
risk factors among a national sample of 15,321 patients. J
Bone Joint Surg Am 2014;96:20-6. Crossref
17. Kuperman EF, Schweizer M, Joy P, Gu X, Fang MM. The
effects of advanced age on primary total knee arthroplasty:
a meta-analysis and systematic review. BMC Geriatr
2016;16:41. Crossref
18. Census and Statistics Department, Hong Kong SAR. Hong
Kong Monthly Digest of Statistics: The mortality trend in
Hong Kong, 1986 to 2018. 2019. Available from: https://www.statistics.gov.hk/pub/B71911FB2019XXXXB0100.pdf. Accessed 20 Sep 2021.
19. Kennedy JW, Johnston L, Cochrane L, Boscainos PJ. Total knee arthroplasty in the elderly: does age affect
pain, function or complications? Clin Orthop Relat Res
2013;471:1964-9. Crossref
20. Williams DP, Price AJ, Beard DJ, et al. The effects of age on patient-reported outcome measures in total knee
replacements. Bone Joint J 2013;95-B:38-44. Crossref