Hong Kong Med J 2021 Oct;27(5):330–7 | Epub 5 Oct 2021
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Burnout and well-being in young doctors in Hong
Kong: a territory-wide cross-sectional survey
Kenny YH Kwan, BMBCh (Oxon), FHKAM (Orthopaedic Surgery)1; Loretta WY Chan, MB, BS, FHKAM (Family Medicine)2; PW Cheng, MB, BS, FHKAM (Psychiatry)3; Gilberto KK Leung, MB, BS (Lon), FHKAM (Surgery)4; CS Lau, MB, ChB (Dundee), FHKAM (Medicine)5; for the Young Fellows Chapter of the Hong Kong Academy of Medicine
1 Department of Orthopaedics and Traumatology, The University of Hong Kong, Hong Kong
2 Family Medicine, Private Practice
3 Department of Psychiatry, The University of Hong Kong, Hong Kong
4 Department of Surgery, The University of Hong Kong, Hong Kong
5 Department of Medicine, The University of Hong Kong, Hong Kong
Corresponding author: Dr Kenny YH Kwan (kyhkwan@hku.hk)
 Full
paper in PDF
Full
paper in PDF
Abstract
Introduction: This territory-wide study evaluated the level of burnout and health status among young doctors in Hong Kong.
Methods: All young doctors in Hong Kong, defined
as residents-in-training or doctors within 10 years
of their specialist registration, were invited to
participate in an online cross-sectional survey.
This survey used standardised questionnaires
including the Copenhagen Burnout Inventory (CBI)
for burnout, Patient Health Questionnaire-9 for
depression, and general health questionnaires.
Results: In total, 514 doctors completed the survey;
284 were doctors within 10 years of their specialist
registration, while 230 were residents-in-training.
There were 277 women (54%); among all respondents,
the mean age was 33.7 ± 6.1 years. Using a CBI subscale
cut-off score of ≥50 (moderate and higher), 72.6%
(n=373) of respondents reported personal burnout;
70.6% (n=363) of respondents reported work-related
burnout; and 55.4% (n=285) of respondents reported
client-related burnout. Furthermore, 24% (n=125) of
respondents were “somewhat dissatisfied” with their
present job position; 4% (n=19) of respondents were
“very dissatisfied” with their present job position.
The prevalence of depression among respondents
was 21% (n=110).
Conclusions: this territory-wide cross-sectional
survey of young doctors in Hong Kong, a high
prevalence of burnout was identified among young
doctors; respondents exhibited a considerable level
of depression and substantial dissatisfaction with
their current positions. Strategies to address these
problems must be formulated to ensure the future
well-being of the medical and dental workforce in
Hong Kong.
New knowledge added by this study
- There is a high prevalence of burnout among young doctors in Hong Kong; of 514 survey respondents, 72.6% reported personal burnout, 70.6% reported work-related burnout, and 55.4% reported client-related burnout.
- The prevalence of depression among young doctors (21% in this study) was considerably higher than among the general population in Hong Kong (8.4% in a previous study).
- Overall, 28% of respondents were either “somewhat dissatisfied” or “very dissatisfied” with their present job position.
- Changes to the number of working hours per week and extent of clinical responsibilities may help to reduce burnout among junior doctors.
- Efforts to promote stronger social networks among junior doctors and their communities may reduce the risk of burnout, although further studies are needed to validate this hypothesis.
- Although the respondents did not indicate reliance on substance or alcohol abuse, there is a need for greater workplace emphasis on positive health and lifestyle behaviours to reduce the risk of burnout among junior doctors.
Introduction
Burnout among doctors is increasingly recognised
as a serious threat to medical and dental practice
across all specialties; its prevalence is increasing worldwide.1 Burnout is a spectrum of clinical
syndromes that were first categorised into three
dimensions by Maslach as emotional exhaustion,
depersonalisation, and a low sense of personal accomplishment.2 Subsequently, it was added to
the International Classification of Diseases as a
syndrome that results from poorly managed chronic
workplace stress.3
Burnout among doctors can lead to decreased
effectiveness and shortening of professional lifespan.4
Burnout exacerbates negative emotions, thereby
impeding cognitive performance; it may result in
biased decision making. Hence, the well-being of
doctors is important for maintaining manpower,
quality of care, and equity of care delivery. Multiple
studies in different countries have shown that the
incidence of burnout among doctors is rising. In
the US, a Medscape nationwide survey showed that
59% of emergency medicine doctors experienced
burnout symptoms, and the incidence had increased
steadily over time.1 In Australia, the National Mental
Health Survey found that the level of very high
psychological distress was significantly greater in
doctors (3.4%) than in the general population (2.6%)
or other professionals (0.7%).5 A cross-sectional
online survey in the United Kingdom also revealed
a high rate of mental health disorders among junior
doctors and medical students.6
To our knowledge, studies regarding well-being
and burnout among doctors in Asia are
limited. Gan et al7 performed a cross-sectional
study of general practitioners in Hubei, China;
they found a combined prevalence of 2.46% across
all three dimensions of emotional exhaustion,
depersonalisation, and personal accomplishment. However, that study only included doctors within a
single specialty in one province. Huang et al8 found
the prevalences of personal burnout and client-related
burnout were 44.0% and 14.8%, respectively,
among residents in Taiwan; however, they used a
non-standardised questionnaire. In Hong Kong, a
previous cross-sectional survey showed that 31.4%
of respondents among doctors in the public sector
had a high rate of burnout, but the sampling criteria
were random and non-specific; moreover, that study
did not include a substantial proportion of doctors
who worked in the private sector.9 Another survey
also suggested that burnout was prevalent among
doctors in Hong Kong, but it only included graduates
from one medical school in Hong Kong.10
Hence, this study aimed to evaluate the
prevalence of burnout in the Hong Kong medical
and dental workforce by administering standardised
questionnaires to a broad population of residents-in-training and doctors within 10 years of their
specialist registration. The study also explored well-being
among doctors in terms of job satisfaction,
depression, lifestyle behaviours, and factors
associated with these states.
Methods
Survey and study population
In this study, all doctors within 10 years of their
specialist registration registered with the Hong
Kong Academy of Medicine, as well as residents-in-training registered with one of the Academy’s
15 constituent Colleges, were invited to complete a
voluntary cross-sectional survey between February
2019 and June 2019. The cut-off of 10 years was
selected because the Hong Kong Academy of
Medicine considers doctors within 10 years of
their specialist registration to be “young Fellows”.
The survey consisted of self-reported demographic
data, year of entry into medical school, and current
professional details. Burnout was assessed using the
validated Copenhagen Burnout Inventory (CBI).11
Depression was assessed using the Patient Health
Questionnaire-9 (PHQ-9).12 Lifestyle factors were
assessed with reference to the respondents’ drinking
habits, sleep patterns, and levels of both exercise
and activities. Items concerning job satisfaction
and lifestyle behaviours were adapted from existing
doctor questionnaires and health surveys.13 14
An online survey was developed in-house by the Hong Kong Jockey Club Innovative Learning
Centre for Medicine of the Hong Kong Academy
of Medicine, then administered electronically.
The invitations to participate were sent via e-mail;
two separate reminder emails were sent after the
initial invitation. As an incentive, respondents were
offered coffee or food coupons after completion of
the survey. The study protocol was approved by the
Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster
(Ref No: UW 19-062).
Sample size calculation
PASS 2000 (NCSS, LLC., Kaysville [UT], US; www.ncss.com) power analysis software was used for
sample size calculation. The prevalence of personal
burnout among young doctors in Hong Kong was
assumed to be similar to the prevalence of personal
burnout among residents in Taiwan (44.0%)8; thus,
to achieve a 95% confidence interval (CI) with a
precision of 4.5%, 458 participants were required.
Our final sample of 514 doctors was sufficient to
achieve the desired statistical power.
Specific instruments
Copenhagen Burnout Inventory
This instrument consists of three scales that measure
personal burnout, work-related burnout, and client-related
burnout; the scales can be applied to workers
in all industries and cultures. Personal burnout
measures the degree of fatigue experienced by the
respondent, irrespective of work experience or
occupational status. Work-related burnout measures
the degree of fatigue related to work; it explores how
the respondent’s perception of work contributes
to fatigue. Client-related burnout is the perceived
degree of fatigue related to work with clients. The
burnout level is calculated as a mean score; therefore,
each scale has a value between 0 and 100. A score of
≥50 indicates a high degree of burnout.15 16 17 18
Patient Health Questionnaire-9
The PHQ-9 is a depression assessment tool, which
scores each of the nine Diagnostic and Statistical
Manual of Mental Disorders IV criteria for
depression on a scale ranging from “0” (not at all)
to “3” (nearly every day). A PHQ-9 score >9 has a
reported sensitivity of 88% and specificity of 88% for
major depression.19
Statistical analysis
The prevalence of burnout is shown using point
estimates and 95% CIs. Descriptive statistics were
presented concerning demographic characteristics
and lifestyle behaviours. Bivariate logistic models
were used to describe the distinct relationships of
suicide, depression, and burnout with demographic,
educational, and professional characteristics. The
data were analysed using SPSS software (Windows
version 26.0; IBM Corp, Armonk [NY], US).
Statistical significance was set at P<0.05.
Results
Participant demographics
There were 746 total respondents; of these, 232 did not complete the entire survey and were excluded
from the analysis. Of the included 514 respondents,
284 were doctors within 10 years of their specialist
registration, while 230 were residents-in-training.
The total number of doctors within 10 years of
their specialist registration invited to participate
in the survey was 2879; thus, the response rate was
estimated as 9.9%. However, it was not possible to
calculate the response rate for residents-in-training.
The respondents included 277 women (54%); the
mean age among all respondents was 33.7 ± 6.1 years.
The respondents’ demographic data are summarised
in Table 1; their current professional statuses are
summarised in Table 2.
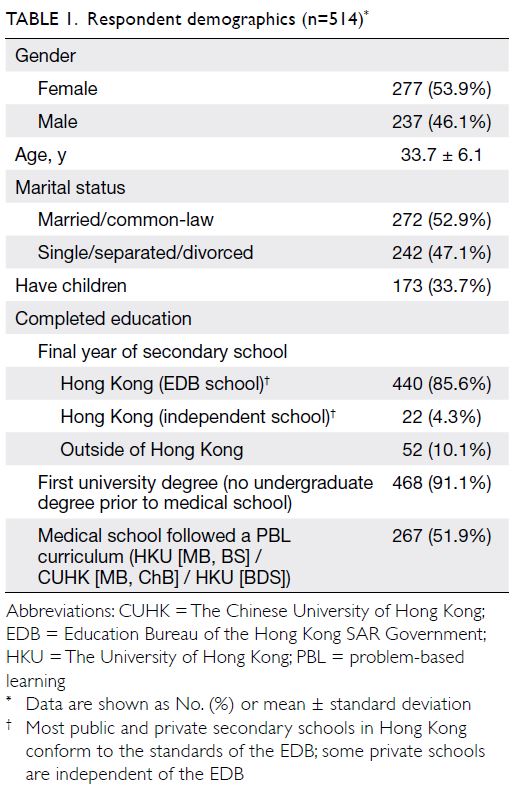
Table 1. Respondent demographics (n=514)
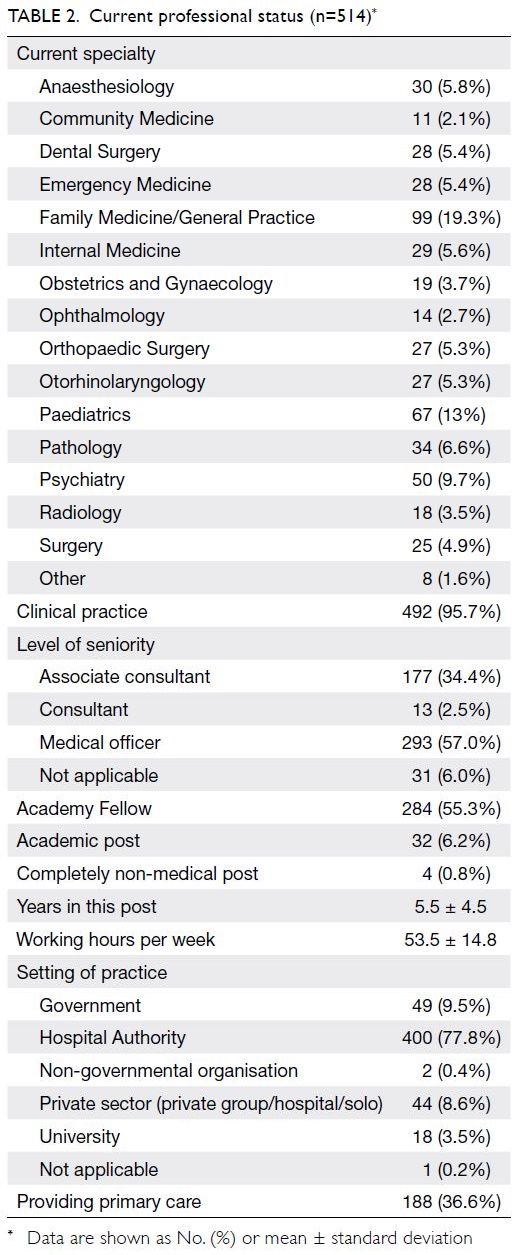
Table 2. Current professional status (n=514)
Professional satisfaction
Overall, 24% (n=125) of respondents were “somewhat dissatisfied” with their present job position, while
4% (n=19) of respondents were “very dissatisfied”
with their present job position. Furthermore, 15%
(n=76) of respondents were “somewhat dissatisfied”
with being a medical doctor, whereas 2% (n=10) of
respondents were “very dissatisfied” with being a
medical doctor. Finally, 3% (n=14) of respondents
indicated they planned to stop practising medicine
in the next 12 months, with stress or burnout (86%)
cited as the most common reason for such plans.
Burnout
As measured by the CBI, the mean personal burnout
score was 59.6 ± 20.5, work-related burnout score
was 57.3 ± 20.1, and client-related burnout score
was 49.0 ± 22.3. Using a CBI subscale cut-off
score of ≥50 (moderate and higher), 72.6% (n=373,
95% CI=68.5%-76.4%) of respondents reported
personal burnout; 70.6% (n=363, 95% CI=66.4%-74.5%) of respondents reported work-related burnout; and 55.4% (n=285, 95% CI=51.0%-59.7%) of respondents reported client-related burnout (Table 3).
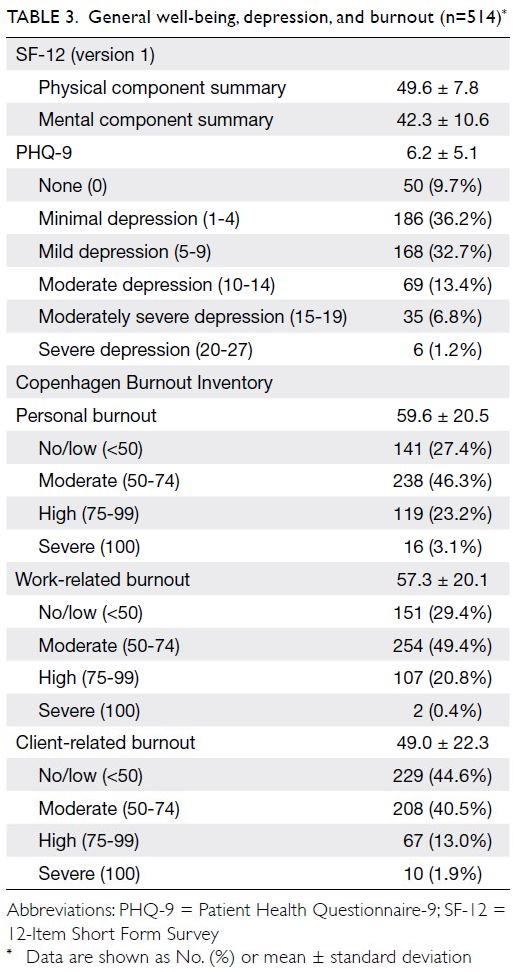
Table 3. General well-being, depression, and burnout (n=514)
Well-being, depression, and suicidal ideation
The mean physical component summary score of the 12-Item Short Form Survey was 49.6 ± 7.8; the mean
mental component summary score of the 12-Item
Short Form Survey was 42.3 ± 10.6 (Table 3).
As measured by the PHQ-9, the mean
depression score was 6.2 ± 5.1. However, the
prevalence of depression among respondents,
defined as a score of ≥10, was 21% (n=110) [Table 3].
In total, 79% (n=404) of respondents did not report any suicidal ideation or attempt. The remaining
respondents stated that life was “not worth living”
or “wished he or she was dead”; some also reported
a history of suicidal ideation or attempts. The most
commonly cited source of stress in the past year was
clinical responsibilities/job demands.
Health status
In terms of health conditions, there was a perception
among respondents that their health status was
“worse” (29%; n=148) or “much worse” (3%;
n=17) than among other individuals of the same
age. The mean duration of sleep each night was
6.2 ± 1.5 hours. However, most respondents
frequently experienced inadequate sleep when at
work; 70% (n=361) of respondents indicated that
this occurred weekly or more often. In terms of
personal habits, the prevalences of alcohol drinking,
drug addiction, and smoking were low. However, the
prevalences of regular physical activity and personal
physical assessments were not high (Table 4).
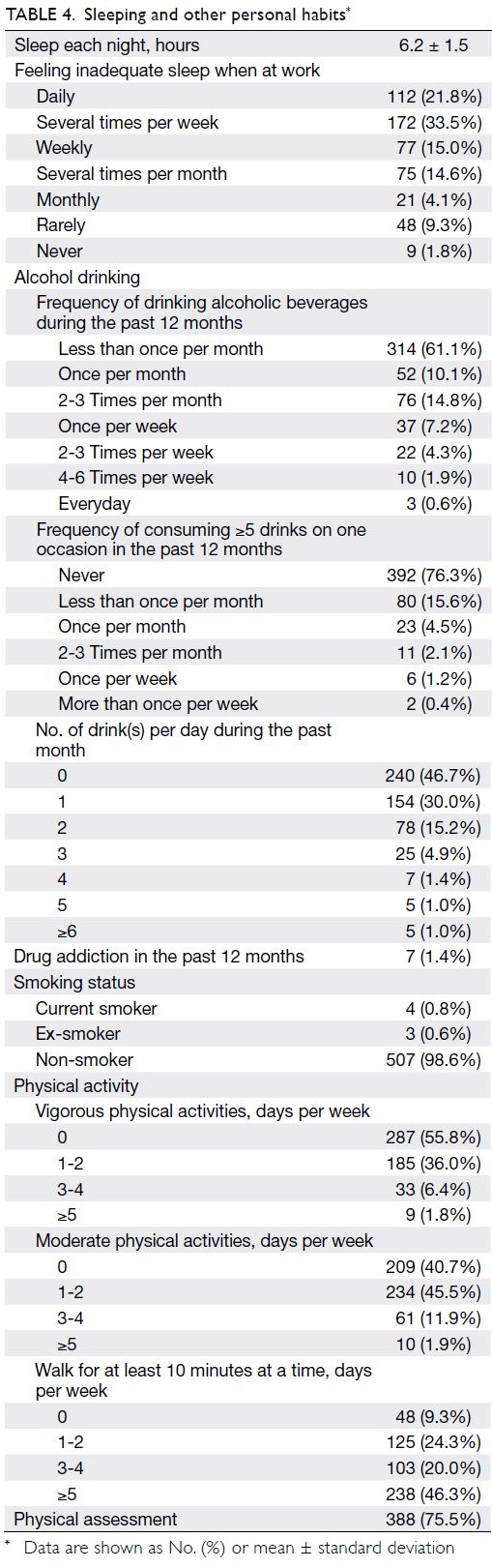
Table 4. Sleeping and other personal habits
Association of factors for burnout,
depression, and suicide
Logistic regression modelling was performed to investigate bivariate associations of demographic
and professional factors with burnout, the presence
of depression, or suicide ideation and/or attempts.
The number of working hour(s) per week
(odds ratio [OR]=1.02; 95% CI=1.01-1.04; P=0.001)
was positively associated with depression (online supplementary Table 1); having children (OR=0.58;
95% CI=0.36-0.93; P=0.024) was negatively associated
with suicidal ideation/attempts. Doctors who
completed a project-based learning curriculum during
undergraduate study were less likely to be depressed
or report suicidal ideation/attempts (depression:
OR=0.60; 95% CI=0.39-0.91; P=0.017; suicidal
ideation/attempts: OR=0.65; 95% CI=0.43-1.00;
P=0.049) [online supplementary Table 2].
Older age (OR=0.97; 95% CI=0.94-0.99;
P=0.026), possession of a first university degree
in medicine or dental surgery (OR=0.37;
95% CI=0.15-0.89; P=0.027), and possession
of Academy fellowship status (OR=0.61;
95% CI=0.41-0.92; P=0.017) were associated with
lower likelihood of personal burnout. Engagement
in longer working hour(s) per week (OR=1.04;
95% CI=1.02-1.05; P<0.001) and working in Hospital
Authority clinics (OR=1.95; 95% CI=1.05-3.62;
P=0.034; compared with working in government
clinics) were positively associated with personal
burnout (online supplementary Table 3). Marital
statuses of single, separated, or divorced (OR=1.71;
95% CI=1.16-2.53; P=0.007) and engagement
in longer working hour(s) per week (OR=1.03;
95% CI=1.02-1.05; P<0.001) were positively
associated with work-related burnout (online supplementary Table 4). Conversely, having children
(OR=0.66; 95% CI=0.44-0.98; P=0.038), consultant
seniority level (OR=0.27; 95% CI=0.09-0.88; P=0.029;
compared with associate consultant seniority
level), and working in the private sector (OR=0.40;
95% CI=0.17-0.94; P=0.035; compared with working
in government) were negatively associated with work-related burnout. Provision of primary care
(OR=1.5; 95% CI=1.04-2.16; P=0.031) was associated
with client-related burnout (online supplementary Table 5).
Discussion
Main findings
This study attempted to quantify well-being and
burnout in young doctors (both resident-in-training,
and doctors within 10 years of their specialist
registration) throughout Hong Kong; there were
three main findings. First, the mean burnout score
was high in this group of doctors; mean personal
and work-related scores of ≥50 were observed on
the CBI. Second, there was a high prevalence of job
dissatisfaction (28%) in this group of doctors. Third,
the self-perceived personal well-being and mental
health were worse in this group of doctors than in
members of the general population with similar ages.
Burnout among doctors in Hong Kong and
worldwide
Burnout is a well-known occupational hazard in
people-oriented professions; doctors are at particular
risk of burnout because of their frequent engagement
in intense personal and emotional contact with
patients. Although these therapeutic and service
relationships are highly rewarding and engaging,
they can also be a source of stress. Burnout among
doctors has been recognised as a global crisis20; its
effects on personal, patient, and institutional levels
can be substantial. The expectation to meet job
demands can lead to maladaptive practices which will
ultimately compromise relationships with patients
and colleagues, with long-term consequences on
patient care.21 Hence, efforts to acknowledge that
such a problem exists represents the first step in
establishing a systematic strategy to address this
crisis.
Although there have been multiple published
reports regarding burnout among doctors, territory-wide
data focusing on junior doctors in Hong Kong are
lacking. Siu et al9 conducted a random sample survey
of 226 public doctors in 2012; they found that 31.4%
of respondents satisfied the criteria for high burnout.
Moreover, young but moderately experienced
doctors needing to work shifts were most vulnerable
to high burnout. However, the questionnaire used
in that study was not comprehensive, the random
sampling method did not produce a representative
cohort, and only public doctors were invited to
the survey. More recently, a more comprehensive
survey involving medical graduates of one university
in Hong Kong found high prevalences of personal
(63.1%) and 55.9% (work-related) burnout using the
standardised CBI.10 The more comprehensive survey represents the most comprehensive and robust study
in Hong Kong thus far, but it only included graduates
from one university in Hong Kong; it did not include
any doctors trained elsewhere.
The present study of young doctors throughout
Hong Kong found high mean personal (59.6 ± 20.5)
and work-related (57.3 ± 20.1) scores on the CBI. The
mean client-related score was 49.0 ± 22.3, slightly
below the score of 50 that constituted the threshold
for burnout. These scores were higher than in the
previous study performed in Hong Kong by Ng et al,10
which showed mean CBI scores of 57.4 ± 21.4
(personal), 48.9 ± 7.4 (work-related), and 41.5 ± 21.8
(client-related). Moreover, when compared with
studies worldwide that used the CBI to measure
burnout in doctors,15 16 18 22 the levels of burnout in the
present study were among the highest. Contributing
factors may differ among regional healthcare
systems; causes of burnout and well-being in junior
doctors may not be consistent worldwide. Our study
attempted to identify sources of stress among junior
doctors in Hong Kong; the most commonly cited
sources were clinical responsibilities/job demands
and professional examinations. Additional in-depth
studies are necessary to determine how these factors
can be modified to alleviate stress in junior doctors.
Health statuses related to burnout risk
The respondents’ general health statuses (in terms of medical conditions) were not substantially worse
than the general population, although 32% of the
respondents indicated self-perceived health worse
than their peers. The present study also showed that
the prevalence of depression was 21%, according to
the PHQ-9. This is more than double the prevalence
previously reported in Hong Kong (8.4%).23 Despite
the high prevalence of depression in the present
study, respondents indicated low rates of suicidal
ideation/attempts. Although a causal relationship
could not be established because of the observational
nature of the study, the number of working hours per
week and having children were factors that affected
risk of depression and suicidal ideation/attempts,
respectively. The mean number of hours worked per
week was 53.5 ± 14.8 hours. Junior doctors who work
>55 hours per week are reportedly twofold more
likely to have frequent health problems (OR=2.05,
95% CI=1.62-2.59; P<0.001) and suicidal ideation
(OR=2.0, 95% CI=1.42-2.82; P<0.001).24 A previous
systemic review showed an association between
long working hours and a depressive state in other
professions in general.25 Positive effects of reduced
working hours among junior doctors have been
found in some studies,26 27 but this relationship is not
consistently observed. For example, in the United
Kingdom, the Working Time Regulations were fully
applied to junior doctors beginning in 2009; these comprised a limit of 48 hours per week, averaged
across a reference period of 26 weeks, with additional
minimum rest periods. However, implementation of
the Working Time Regulations has not fully resolved
the effects of long hours and fatigue.28 Furthermore,
there are implications for professional training and
manpower planning if rigid enforcement of such
working hours is performed.
Our study did not find any substantial evidence
that young doctors were reliant on alcohol, smoking,
or drugs as coping mechanisms. This contrasts with
findings from the US, which indicated that high levels
of alcohol and substance abuse were associated with
burnout among doctors.29 It was beyond the scope
of the present study to explore other avenues that
junior doctors in Hong Kong might use to alleviate
their stress levels and burnout. Other health and
lifestyle behaviours (eg, exercise levels and personal
physical assessments) may be indicative of time
constraints related to work or personal obligations;
they may also be indicative of self-neglect caused by
such constraints and work-related burnout.
Limitations
This study had several limitations. First, it was a cross-sectional study with voluntary participation,
and the results might not be representative of all
doctors throughout public and private sectors in
Hong Kong. However, to our knowledge, this study
performed the most comprehensive survey regarding
burnout among doctors in Hong Kong thus far.
Second, the study was not designed to avoid selection
bias concerning doctors who were more prone to
burnout and therefore more interested to participate
in such surveys. Third, because the survey did not
allow free text entry in the questionnaire responses,
more in-depth analysis was not possible in some
instances. Fourth, because this was a cross-sectional
survey, no causal relationships or risk factors could
be established regarding the development of burnout
or depression. Fifth, our definition of “young” was
based on the 10 years of specialist registration, which
included doctors with various levels of experience
and responsibilities; thus, the results might not be
representative of a specific subset of doctors.
Conclusions
The present study showed that junior doctors in Hong Kong had a high level of burnout, and
there was a high prevalence of depression among
the respondents. A substantial proportion of the
respondents were dissatisfied with their present job
position. Future studies to determine causal factors
will allow the development and implementation of
specific strategies to address these problems within
Hong Kong. The maintenance of well-being in junior
doctors is vital for sustaining a healthy medical
workforce and long-term patient care.
Author contributions
Concept or design: All authors.
Acquisition of data: KYH Kwan, LWY Chan, PW Cheng.
Analysis or interpretation of data: KYH Kwan, LWY Chan, PW Cheng.
Drafting of the manuscript: KYH Kwan.
Critical revision of the manuscript for important intellectual content: All authors.
Acquisition of data: KYH Kwan, LWY Chan, PW Cheng.
Analysis or interpretation of data: KYH Kwan, LWY Chan, PW Cheng.
Drafting of the manuscript: KYH Kwan.
Critical revision of the manuscript for important intellectual content: All authors.
Conflicts of interest
The authors have no conflicts of interest to disclose.
Acknowledgement
The authors thank all members of the Young Fellows Chapter
of the Hong Kong Academy of Medicine for their active
participation in this study; the secretariat and staff of the
Hong Kong Academy of Medicine and its Hong Kong Jockey
Club Innovative Learning Centre for Medicine for their
administrative and information technology support; and the
Council of the Hong Kong Academy of Medicine for their
active support, encouragement, and funding of the coupons.
The authors especially thank Dicken CC Chan for statistical
assistance.
Funding/support
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This study was approved by the Institutional Review Board of The University of Hong Kong/Hospital Authority Hong Kong West Cluster (Ref No: UW 19-062).
References
1. Kane L. Medscape national physician burnout and
depression report 2019. Available from: https://www.medscape.com/slideshow/2019-lifestyle-burnout-depression-6011056. Accessed 2 Dec 2020.
2. Maslach C. What have we learned about burnout and health? Psychol Health 2001;16:607-11.Crossref
3. World Health Organization. International Classification of Diseases 11th Revision. QD85 Burnout. Available from:
https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/129180281. Accessed 3 Dec 2020.
4. Lin M, Battaglioli N, Melamed M, Mott SE, Chung AS,
Robinson DW. High prevalence of burnout among US
emergency medicine residents: results from the 2017
National Emergency Medicine Wellness Survey. Ann
Emerg Med 2019;74:682-90. Crossref
5. BeyondBlue. National Mental Health Survey of Doctors
and Medical Students 2019. Available from: https://www.beyondblue.org.au/docs/default-source/beyond-blue-s-strategic-plan-2020-2023/research-project-files/bl1132-report---nmhdmss-full-report_web.pdf?sfvrsn=845cb8e9_14. Accessed 3 Dec 2020.
6. Bhugra D, Sauerteig SO, Bland D, et al. A descriptive study
of mental health and wellbeing of doctors and medical
students in the UK. Int Rev Psychiatry 2019;31:563-8. Crossref
7. Gan Y, Jiang H, Li L, et al. Prevalence of burnout and
associated factors among general practitioners in Hubei,
China: a cross-sectional study. BMC Public Health 2019;19:1607. Crossref
8. Huang EC, Pu C, Huang N, Chou YJ. Resident burnout in Taiwan Hospitals—and its relation to physician felt trust from patients. J Formos Med Assoc 2019;118:1438-49. Crossref
9. Siu CF, Yuen SK, Cheung A. Burnout among public doctors in Hong Kong: cross-sectional survey. Hong Kong Med J 2012;18:186-92.
10. Ng AP, Chin WY, Wan EY, Chen J, Lau CS. Prevalence and severity of burnout in Hong Kong doctors up to 20
years post-graduation: a cross-sectional study. BMJ Open
2020;10:e040178. Crossref
11. Kristensen TS, Borritz M, Villadsen E, Christensen KB.
The Copenhagen Burnout Inventory: a new tool for the
assessment of burnout. Work Stress 2005;19:192-207. Crossref
12. Rizzo R, Piccinelli M, Mazzi MA, Bellantuono C, Tansella M.
The Personal Health Questionnaire: a new screening
instrument for detection of ICD-10 depressive disorders in
primary care. Psychol Med 2000;30:831-40. Crossref
13. Heponiemi T, Kouvonen A, Vänskä J, et al. Health,
psychosocial factors and retirement intentions among
Finnish physicians. Occup Med (Lond) 2008;58:406-12. Crossref
14. Taylor K, Lambert T, Goldacre M. Future career plans of
a cohort of senior doctors working in the National Health
Service. J R Soc Med 2008;101:182-90. Crossref
15. Benson S, Sammour T, Neuhaus SJ, Findlay B, Hill AG. Burnout in Australasian younger fellows. ANZ J Surg
2009;79:590-7. Crossref
16. Chou LP, Li CY, Hu SC. Job stress and burnout in hospital employees: comparisons of different medical professions in a regional hospital in Taiwan. BMJ Open 2014;4:e004185. Crossref
17. Creedy DK, Sidebotham M, Gamble J, Pallant J, Fenwick J.
Prevalence of burnout, depression, anxiety and stress
in Australian midwives: a cross-sectional survey. BMC
Pregnancy Childbirth 2017;17:13. Crossref
18. Wright JG, Khetani N, Stephens D. Burnout among faculty
physicians in an academic health science centre. Paediatr Child Health 2011;16:409-13. Crossref
19. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med 2001;16:606-13. Crossref
20. Physician burnout: a global crisis [editorial]. Lancet 2019;394:93. Crossref
21. Graham J, Potts HW, Ramirez AJ. Stress and burnout in doctors. Lancet 2002;360:1975-6. Crossref
22. Thomas LR, Ripp JA, West CP. Charter on physician well-being.
JAMA 2018;319:1541-2. Crossref
23. Cheng CM, Cheng M. To validate the Chinese version of
the 2Q and PHQ-9 questionnaires in Hong Kong Chinese
patients. HK Pract 2007;29:381-90.
24. Petrie K, Crawford J, LaMontagne AD, et al. Working
hours, common mental disorder and suicidal ideation
among junior doctors in Australia: a cross-sectional survey.
BMJ Open 2020;10:e033525. Crossref
25. Bannai A, Tamakoshi A. The association between
long working hours and health: a systematic review of
epidemiological evidence. Scand J Work Environ Health
2014;40:5-18. Crossref
26. Kiernan M, Civetta J, Bartus C, Walsh S. 24 Hours on-call
and acute fatigue no longer worsen resident mood under
the 80-hour work week regulations. Curr Surg 2006;63:237-41. Crossref
27. Kort KC, Pavone LA, Jensen E, Haque E, Newman N,
Kittur D. Resident perceptions of the impact of work-hour
restrictions on health care delivery and surgical education:
time for transformational change. Surgery 2004;136:861-71. Crossref
28. Morrow G, Burford B, Carter M, Illing J. Have restricted
working hours reduced junior doctors' experience of
fatigue? A focus group and telephone interview study. BMJ
Open 2014;4:e004222. Crossref
29. Oreskovich MR, Shanafelt T, Dyrbye LN, et al. The
prevalence of substance use disorders in American
physicians. Am J Addict 2015;24:30-8. Crossref