© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
LETTER TO THE EDITOR
Febrile seizures in children: a condensed update
MM Yau, FHKAM (Paediatrics)1; KL Hon,
MD, FAAP2; CF Cheng, FHKAM (Paediatrics)3
1 Department of Paediatrics and
Adolescent Medicine, Tseung Kwan O Hospital, Tseung Kwan O, Hong Kong
2 Department of Paediatrics and
Adolescent Medicine, Hong Kong Children’s Hospital, Kowloon Bay, Hong Kong
3 Private Practice
Corresponding author: Dr MM Yau (yaumanmut@gmail.com)
 Full
paper in PDF
Full
paper in PDF
To the Editor—We would like to provide a
condensed update on febrile seizures in children.
Febrile seizures are the most common type of
provoked seizure in children. The cumulative risk varies in different
cohorts but is generally reported from 2% to 5%.1
The typical febrile seizure is a generalised short seizure provoked by a
febrile episode in children aged 6 months to 6 years. The duration is
shorter than 15 minutes and usually does not recur in the same episode.
There are typically no focal neurological deficits or signs of central
nervous system (CNS) infection.2
Acute management of convulsive seizures, such as resuscitation and
first-aid measures, should follow the local prevailing guideline provided
by the Hospital Authority intranet.
Diagnosing typical febrile seizure is clinically
important and can follow a simple management pathway (Fig).
The chance of CNS infection and long-term neurodevelopmental sequelae is
low. There is no significant difference in academic performance and
behaviour at age 10 years for children who had a typical or atypical
febrile seizure compared with control.3
Further tests are necessary for fever rather than the seizures themselves.
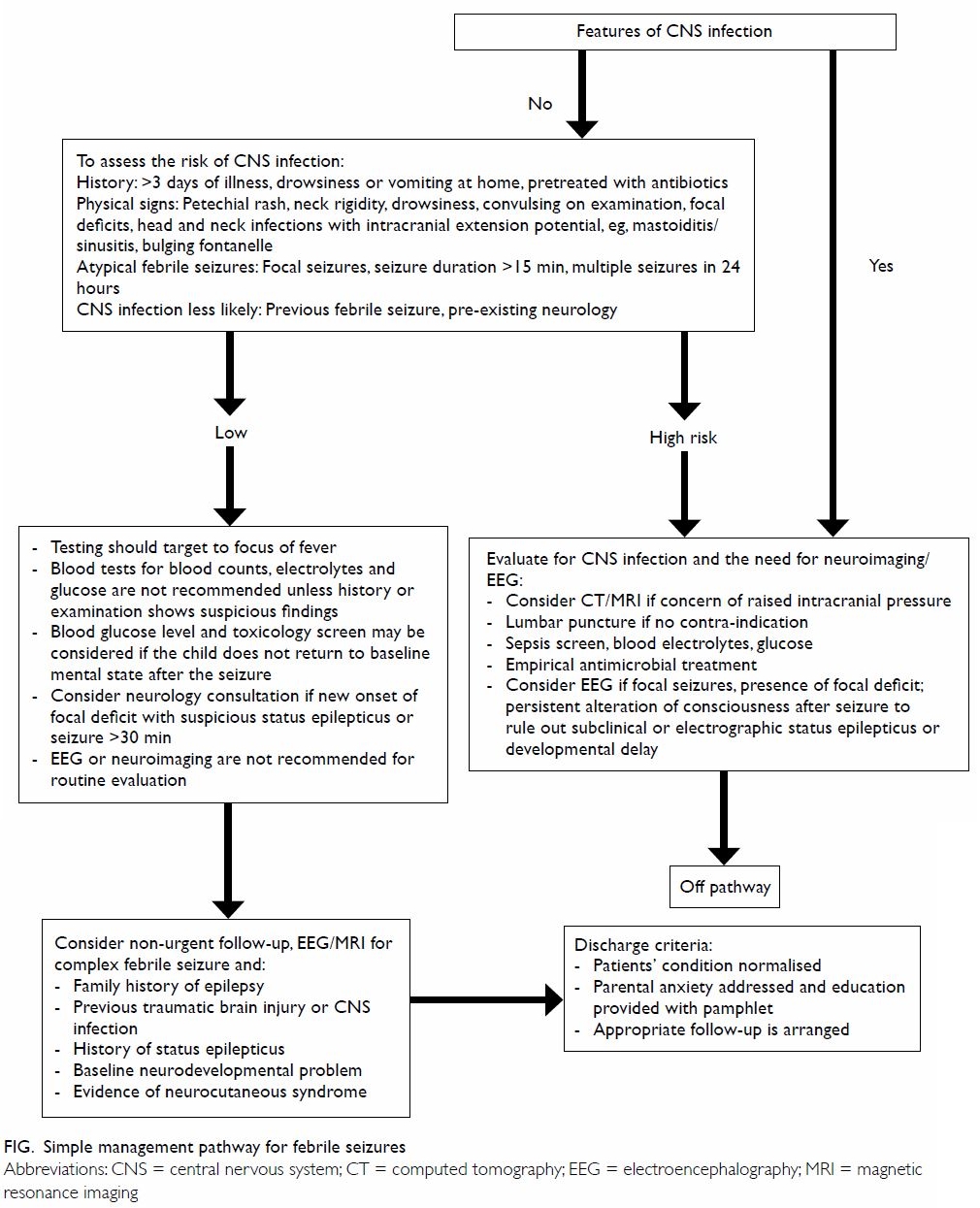
Figure. Simple management pathway for febrile seizures
Lumbar puncture to exclude CNS infection is
unnecessary even in infants aged <1 year with simple febrile seizures.
It should be considered in complex febrile seizures, prolonged seizures,
or presence of red flag signs such as meningism, bulging fontanelle, or
focal neurological deficit.
Urgent neuroimaging, such as computer tomography or
magnetic resonance imaging, should be considered only in prolonged
seizures, presence of focal neurological deficits, or prolonged
encephalopathic state.
Electroencephalography is of limited value even in
complex febrile seizures. It might be considered in focal seizures,
presence of focal deficit, persistent alteration of consciousness after
seizure (to rule out subclinical or electrographic status epilepticus), or
developmental delay.
Counselling is the most important aspect in
managing febrile seizures:
1. Prognosis: excellent prognosis for typical
febrile seizure; no significant increase in future epilepsy or other
neurodevelopmental sequelae for typical febrile seizure even if recurrent;
higher risk of sequelae in the presence of atypical features.4
2. Recurrence risk: on average 30% before 6 years old, higher if first attack at a younger age or in the presence of atypical features.
3. Antipyretics are not recommended for febrile seizure prophylaxis.
4. Long-term or intermittent anticonvulsants are useful to reduce recurrence but in general not recommended because of their side-effects.
5. Rescue medication, eg, rectal diazepam should be considered for prolonged febrile seizure, febrile status epilepticus, or patients with limited medical access.
6. Intermittent oral benzodiazepines could be considered for recurrent febrile seizures which are likely predictable, ie, seizures occurred after detection of fever.
7. Caregivers should be taught to manage acute seizures.
2. Recurrence risk: on average 30% before 6 years old, higher if first attack at a younger age or in the presence of atypical features.
3. Antipyretics are not recommended for febrile seizure prophylaxis.
4. Long-term or intermittent anticonvulsants are useful to reduce recurrence but in general not recommended because of their side-effects.
5. Rescue medication, eg, rectal diazepam should be considered for prolonged febrile seizure, febrile status epilepticus, or patients with limited medical access.
6. Intermittent oral benzodiazepines could be considered for recurrent febrile seizures which are likely predictable, ie, seizures occurred after detection of fever.
7. Caregivers should be taught to manage acute seizures.
Author contributions
All authors have made substantial contributions to
the concept of this study, acquisition and analysis of data, drafting of
the article, and critical revision for important intellectual content. All
authors had full access to the data, contributed to the study, approved
the final version for publication, and take responsibility for its
accuracy and integrity.
Conflicts of interest
All authors have disclosed no conflicts of
interest.
Funding/support
This letter received no specific grant from any
funding agency in the public, commercial, or not-for-profit sectors.
References
1. Chan KK, Cherk SW, Chan CH, Ng DK, Ho
JC. A retrospective review of first febrile convulsion and its risk
factors for recurrence in Hong Kong children. HK J Paediatr 2007;12:181-7.
2. Wong V, Ho MH, Rosman NP, et al.
Clinical guideline on management of febrile convulsion. HK J Paediatr
2002;7:143-51.
3. Verity CM, Greenwood R, Golding J.
Long-term intellectual and behavioral outcomes of children with febrile
convulsions. N Engl J Med 1998;338:1723-8. Crossref
4. Leung AK, Hon KL, Leung TN. Febrile
seizures: an overview. Drugs Context 2018;7:212536. Crossref