Hong
Kong Med J 2019 Dec;25(6):490.e1-2
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Ruptured ovarian teratoma with granulomatous
peritonitis
WL Wong, MB, BS, FRCR1; Anthony WT
Chin, MB, ChB, FRCR1; WM Yu, MB, ChB1; FH Ng, FRCR,
FHKAM (Radiology)2
1 Department of Radiology, United
Christian Hospital, Kwun Tong, Hong Kong
2 Department of Radiology, Caritas
Medical Centre, Shamshuipo, Hong Kong
Corresponding author: Dr WL Wong (jesswong723@gmail.com)
 Full
paper in PDF
Full
paper in PDF
Case
In January 2017, a 35-year-old woman was admitted
to our hospital with insidious onset of upper abdominal pain. A computed
tomography (CT) scan showed bilateral ovarian cysts with fat fluid level,
calcifications, and Rokitansky protuberance, compatible with ovarian
teratoma (Fig 1). Anti-dependent fatty pockets with soft
tissue rim were found at the bilateral subphrenic space, likely
representing reactive changes to spilt cyst content, which also explained
the patient’s upper abdominal pain. The patient had stable vital signs and
was therefore treated conservatively. Follow-up ultrasonography scan
showed globular fatty locules on the liver surface, compatible with
escaped fatty cyst content (Fig 2). Subsequently, the patient underwent
bilateral ovarian cystectomy. Histology confirmed bilateral ovarian mature
cystic teratoma. Intra-operatively, widespread flimsy adhesions and
multiple sebum-like implants were seen in the peritoneal cavity,
consistent with changes related to teratoma rupture. The peritoneal cavity
was irrigated and her symptoms gradually subsided; however, follow-up CT
showed mild interval enlargement of the fat-attenuated lesions (Fig
3).
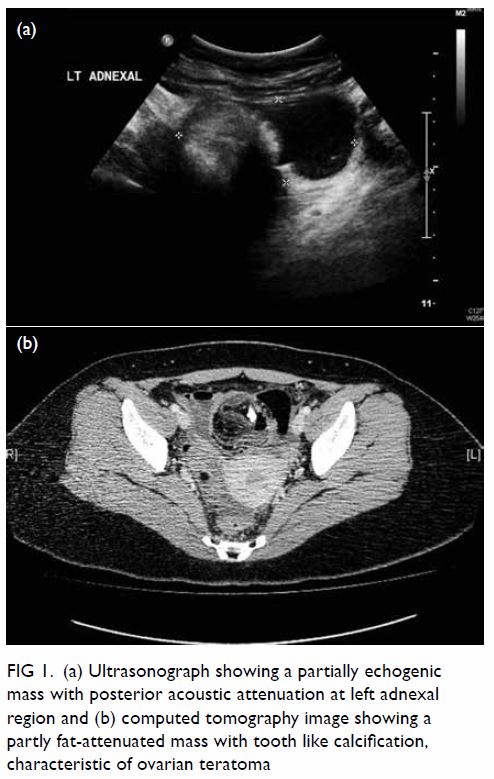
Figure 1. (a) Ultrasonograph showing a partially echogenic mass with posterior acoustic attenuation at left adnexal region and (b) computed tomography image showing a partly fat-attenuated mass with tooth like calcification, characteristic of ovarian teratoma
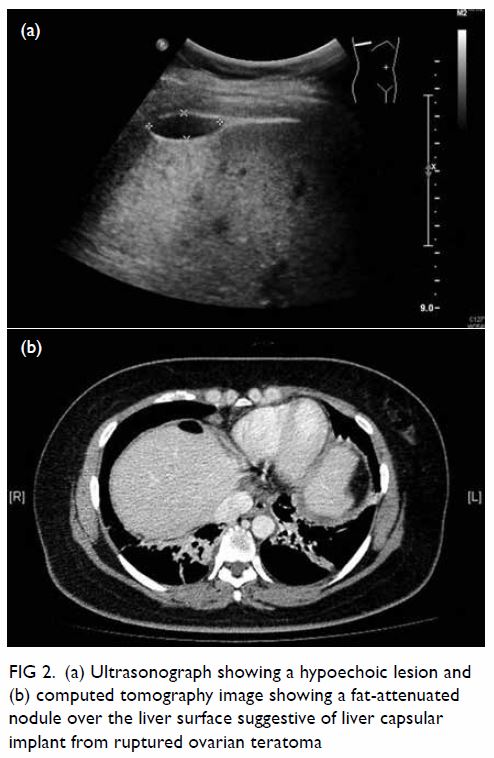
Figure 2. (a) Ultrasonograph showing a hypoechoic lesion and (b) computed tomography image showing a fat-attenuated nodule over the liver surface suggestive of liver capsular implant from ruptured ovarian teratoma
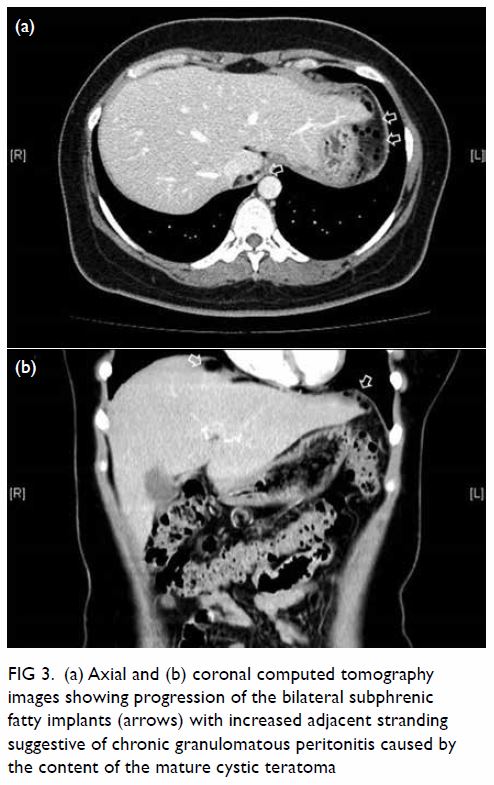
Figure 3. (a) Axial and (b) coronal computed tomography images showing progression of the bilateral subphrenic fatty implants (arrows) with increased adjacent stranding suggestive of chronic granulomatous peritonitis caused by the content of the mature cystic teratoma
Discussion
Mature cystic teratomas (also known as dermoid
cysts) are common ovarian germ cell neoplasms accounting up to 10% to 25%
of all ovarian neoplasms.1 They are
cystic tumours composed of well-differentiated derivations from at least
two of the three germ cell layers. Tumours are bilateral in about 10% of
cases. On ultrasonography, cystic teratoma commonly manifests as a cystic
lesion with a densely echogenic tubercle projecting into the cystic lumen;
or a diffusely or partially echogenic mass with posterior attenuation by
sebaceous material and hair. Multiple thin echogenic bands caused by hair
in cyst cavity can also been seen. Pure sebum within the cyst can be
hypoechoic or anechoic, fluid-fluid level can result from sebum floating
on aqueous fluid which appears more echogenic than the sebum layer. On CT,
the diagnosis of mature cystic teratoma is rather straightforward; fat
attenuation within a cyst is diagnostic of mature cystic teratoma. Teeth
or other calcifications can be seen in 56% of cases.2
Spontaneous rupture is an uncommon complication of
dermoid cysts owing to the presence of a thick capsule, and is only seen
in 1% to 4% of cases.1 Acute
peritonitis can result from sudden rupture of tumour contents as seen in
the present case. Chronic granulomatous peritonitis is caused by
chronically leaking teratoma and is characterised by multiple small white
peritoneal implants and dense adhesions with variable ascites.
Visualisation of fatty implants within the peritoneal cavity is
diagnostic.3
The reported CT findings of granulomatous
peritonitis or intraperitoneal rupture of teratoma are inconsistent.1 3 In one case,
capsular fatty implants were seen in the dome of the liver, similar to the
CT appearance in the present case. In other patients there can be a
significant amount of intraperitoneal free fluid and an omental cake
appearance mimicking peritoneal carcinomatosis.
Chronic granulomatous peritonitis is a potentially
serious complication of ruptured dermoid cyst and can lead to bowel
obstruction resulting from adhesion. Removal of cystic content and copious
peritoneal lavage should be performed to prevent new adhesion and
peritoneal granuloma, and can be a successful method for treating chemical
peritonitis caused by ruptured ovarian teratoma.4
In the present case, progression of the right subphrenic fatty implant,
possibly related to incomplete removal of the cystic content, resulted in
chronic granulomatous peritonitis. The patient may have benefitted from
further peritoneal lavage.
Author contributions
WL Wong contributed to acquisition of data. All
authors contributed to concept or design, analysis or interpretation of
data, drafting of the article, and critical revision for important
intellectual content. All authors had full access to the data, contributed
to the study, approved the final version for publication, and take
responsibility for its accuracy and integrity.
Conflicts of interest
All authors have disclosed no conflicts of
interest.
Funding/support
This research received no specific grant from any
funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This study was approved by the Kowloon
Central/Kowloon East Research Ethics Committee (Ref KC/KE-19-0158/ER-4).
Informed consent was obtained from the patient.
References
1. Erbay G. Ruptured ovarian dermoid cyst
mimicking peritoneal carcinomatosis: CT and MRI. J Clin Anal Med
2016;6:701-3.
2. Outwater EK, Siegelman ES, Hunt JL.
Ovarian teratomas: tumor types and imaging characteristics. Radiographics
2001;21:475-90. Crossref
3. Fibus TF. Intraperitoneal rupture of a
benign cystic ovarian teratoma: findings at CT and MR imaging. AJR Am J
Roentgenol 2000;174:261-2. Crossref
4. Shamshirsaz AA, Shamshirsaz AA, Vibhaka
JL, Broadwell C, Van Voorhis BJ. Laparoscopic management of chemical
peritonitis caused by dermoid cyst spillage. JSLS 2011;15:403-5. Crossref