© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
CASE REPORT
Per urethral insertion of foreign body for erotism:
case reports
Christy WH Mak, MB, ChB; CL Cho, FRCSEd (Urol),
FHKAM (Surgery); Wayne KW Chan, FRCSEd (Urol), FHKAM (Surgery); Ringo WH
Chu, FRCSEd (Urol), FHKAM (Surgery); IC Law, FRCSEd (Urol), FHKAM
(Surgery)
Division of Urology, Department of Surgery, Kwong
Wah Hospital, Yaumatei, Hong Kong
Corresponding author: Dr CL Cho (chochaklam@yahoo.com.hk)
 Full
paper in PDF
Full
paper in PDF
Case reports
Patient 1
A 31-year-old man presented in December 2016 with a
1-day history of retained foreign body in the urinary bladder. He reported
regular insertion of a commercially available silicone urethral instrument
for autoerotism. He customarily evacuated the instrument by voiding but he
had failed to do so on this occasion. There was no dysuria, haematuria,
abdominal pain or fever. Laboratory parameters were within normal limits
and no foreign body could be identified on X-ray. Flexible cystoscopy
revealed an 18-cm length of soft tubing inside the urinary bladder (Fig
1a). Successful retrieval was achieved with endoscopic forceps. He
was discharged home on the same day.
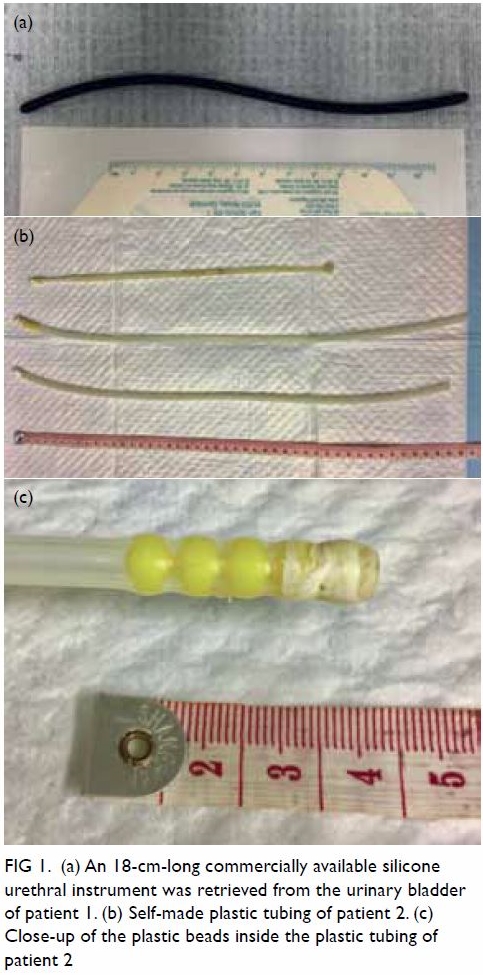
Figure 1. (a) An 18-cm-long commercially available silicone urethral instrument was retrieved from the urinary bladder of patient 1. (b) Self-made plastic tubing of patient 2. (c) Close-up of the plastic beads inside the plastic tubing of patient 2
Patient 2
A 57-year-old man was admitted in January 2017 with
a 6-week history of intermittent fever and right scrotal swelling. He had
no lower urinary tract symptoms except for a yellowish urethral discharge.
He revealed a history of regular per urethral insertion of self-customised
plastic tubing with plastic beads inside the lumen for sexual
gratification (Fig 1b and c). The patient cleaned the tubing with
tap water after each use. Physical examination revealed a tender and
swollen right testis with fluctuance, indicative of abscess formation.
Serum white blood cell count was 15.1 × 109/L. Drainage of
scrotal abscess was performed and the patient was discharged home with a
course of antibiotics.
Patient 3
A 55-year-old woman was admitted in May 2017 with a
1-day history of retained vibrator in the urinary bladder. The vibrator
was inserted into her urethra during sexual activity with her husband. She
complained of subsequent dysuria and haematuria. Serum white blood cell
count was mildly elevated. X-ray revealed a 12.5-cm foreign body in the
pelvic region (Fig 2). Retrieval of the vibrator via flexible
cystoscopy failed owing to inadequate size and strength of the cystoscopic
forceps. Semi-rigid ureteroscopy was used to locate the vibrator with
Kocher forceps placed alongside for removal. Removal of the vibrator was
achieved and the patient was discharged home with antibiotics.

Figure 2. X-ray shows vibrator in pelvic region of patient 3
Discussion
Polyembolokoilamania refers to the act of inserting
a foreign body into body orifices. Urethral polyembolokoilamania is not
uncommon and several cases have been reported in the literature. Different
types of foreign bodies have been reportedly introduced into the urethra,
including electric wires, thermometers, hairpins, toothpicks, eyeglass
rims, straws, pencils, paperclips, and fishhooks.1
2 Autoerotism is one of the most
common reasons given for polyembolokoilamania, although others include
curiosity, psychiatric illness, iatrogenic causes, and an attempt to
relieve urinary symptoms.3 The
prevalence of the condition is unknown and probably underreported owing to
embarrassment of patients so a high index of suspicion and targeted
history taking play an important role in correctly diagnosing the
condition. There are reports suggesting the possible role of psychiatric
assessment in revealing an underlying psychiatric disease and preventing
repeated occurrences of foreign body insertion.4
Nonetheless psychiatric assessment is not considered mandatory for all
patients. The prevalence of psychiatric diagnoses in this group of
patients and the efficacy of psychiatric interventions are still largely
unknown. There is no consensus on the role of psychiatric consultation for
patients with urethral polyembolokoilamania.
Various complications may arise from insertion of
foreign bodies per urethra including urinary tract infection, urethral
injury and, most commonly, retained foreign body. The presentation of
retained foreign body in the lower urinary tract varies widely although
dysuria and haematuria are the most common presentation.3 5 The severity
of the condition depends on the nature of the foreign body and, more
importantly, time to medical attention. Early diagnosis and removal of the
foreign body are of prime importance. In our case series, patients 1 and 3
sought early medical advice and experienced no complications. Late
presentation may lead to complications such as recurrent urinary tract
infection and urolithiasis or, less commonly, erosion of foreign body to
adjacent organs.5 Presenting time
is highly variable, ranging from hours to months.1
Delay in seeking medical consultation may stem from ignorance, psychiatric
illness, or embarrassment.1
X-ray is often performed but is helpful in
identifying only radio-opaque objects. Instead, flexible cystoscopy should
be performed early for all patients with suspected retained foreign body
in the lower urinary tract, in view of the relative simplicity and low
risk of the procedure. Flexible cystourethroscopy can achieve accurate
diagnosis and treatment simultaneously. A high success rate of 50% to 93%
has been reported for endoscopic removal of foreign body.1 3 Computed
tomography scan is indicated only in patients with peritonitis or
suspected foreign body migration to adjacent organs.3
A surgical approach for retrieval of retained
foreign body depends on the size, shape and location of the object. Simple
measures, for example milking of the urethra, usually have a high success
rate for expulsion of foreign body located in the distal penile urethra.3 Invasive approaches including open
cystostomy and perineal urethrostomy have been reported when retrieving
larger size, encrusted, or sharp objects after failed endoscopic
manoeuvres.1 More complex
procedures, including laparotomy and urinary diversion may be indicated
for complicated cases. The surgical approach should be individualised.5
Insertion of foreign bodies into the urethra is
predominantly reported in men. Palmer et al3 reported that 97% of their
patients were men during their 15 years’ experience of managing
self-insertion of urethral foreign bodies and six of their 27 patients had
a recurrent history. This male-dominated phenomenon is also evidenced by
the wide availability of male sexual urethral instruments in shops and
online platforms. These instruments, namely urethral sounds and dilators,
generally constitute a 15- to 20- cm-long stainless steel or silicone tube
that is used for deep penetration to the level of the prostatic urethra.
Deep prostate stimulation-associated orgasms are thought to be more
intense than those with direct penile stimulation, and involve more pelvic
muscle contractions.6 However,
hygiene of the instrument is a concern as instrumentation without proper
disinfection subjects a patient to further risk of infective
complications.
In conclusion, insertion of a foreign body into the
lower urinary tract for erotism is not uncommon, especially in men. Early
diagnosis and endoscopic removal of the foreign body achieve a high
success rate and should be considered the initial management. Delayed
presentation may lead to complications that require further imaging and
more complex surgical procedures.
Author contributions
All authors had full access to the data,
contributed to the study, approved the final version for publication, and
take responsibility for its accuracy and integrity.
Concept or design: CL Cho.
Acquisition of data: CWH Mak.
Analysis or interpretation of data: CL Cho, CWH Mak.
Drafting of the article: CWH Mak, CL Cho.
Critical revision for important intellectual content: All authors.
Acquisition of data: CWH Mak.
Analysis or interpretation of data: CL Cho, CWH Mak.
Drafting of the article: CWH Mak, CL Cho.
Critical revision for important intellectual content: All authors.
Conflicts of interest
The authors have disclosed no conflict of interest.
Funding/support
This research received no specific grant from any
funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
Verbal consent was obtained for the purpose of case
study.
References
1. Rafique M. Intravesical foreign bodies:
review and current management strategies. Urol J 2008;5:223-31.
2. Rahman NU, Elliott SP, McAninch JW.
Self-inflicted male urethral foreign body insertion: endoscopic management
and complications. BJU Int 2004;94:1051-3. Crossref
3. Palmer CJ, Houlihan M, Psutka SP, Ellis
KA, Vidal P, Hollowell CM. Urethral foreign bodies: clinical presentation
and management. Urology 2016;97:257-60. Crossref
4. Unruh BT, Nejad SH, Stern TW, Stern TA.
Insertion of foreign bodies (polyembolokoilamania): underpinnings and
management strategies. Prim Care Companion CNS Disord 2012;14(1). pii:
PCC.11f01192. Crossref
5. Cury J, Coelho RF, Srougi M.
Retroperitoneal migration of a self-inflicted ballpoint pen via the
urethra. Int Braz J Urol 2006;32:193-5. Crossref
6. Alwaal A, Breyer BN, Lue TF. Normal male
sexual function: emphasis on orgasm and ejaculation. Fertil Steril
2015;104:1051-60. Crossref