© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
REMINISCENCE: ARTEFACTS FROM THE HONG KONG MUSEUM OF MEDICAL SCIENCES
The Brook airway: a life-saving device
TW Wong, FHKAM (Emergency Medicine)
Member, Education and Research Committee, Hong Kong Museum of Medical Sciences Society
 Full
paper in PDF
Full
paper in PDF
The cardiopulmonary resuscitation (CPR) technique,
as we know it today, was popularised during the
1960s. It had two components: mouth-to-mouth
ventilation and closed chest compression. Mouth-to-mouth
artificial breathing was not something new as
it was reported in the 18th century.1 Its use faded away
over the next two centuries because of the advent of
the germ theory and the belief that expired air was
unsuitable for resuscitation due to the presence of
carbon dioxide and a low oxygen concentration.2 In
the 19th century, various manual methods of artificial
ventilation were introduced and taught in first-aid
courses. James Elam, an anaesthetist from the United
States, was credited with reviving the use of mouth-to-mouth breathing in the 1950s. He demonstrated
with experiments in the operating theatre that expired
air could be used to maintain adequate arterial oxygen
saturation.3 Peter Safar, a contemporary of Elam,
also demonstrated that even laymen could be taught
to open the airway and provide adequate mouth-to-mouth ventilation in adults. He also found that
the traditional manual methods of ventilation were
ineffective to maintain oxygenation.4 5 Thus, the stage was set to introduce the kiss of life. Mouth-to-mouth
artificial ventilation in adults was endorsed by the
American Medical Association in 1958. Meanwhile,
a team from Johns Hopkins University wrote about
the effectiveness of closed-chest compression in
maintaining perfusion following cardiac arrest.6 The
term “cardiopulmonary resuscitation” was coined by
the American Heart Association in 1962 and CPR
training was gradually introduced.
Although the efficacy of mouth-to-mouth
ventilation is not in doubt, it may not be acceptable
to many. There are psychological barriers to applying
the lips on a moribund person, especially when there
may be vomitus and other secretions present. Some
form of barrier device is thus desirable. Morris Brook
(1911-1967), a general practitioner from Saskatoon,
Canada, was involved in the resuscitation of a miner
during a cave-in in 1957. This man was unconscious
and not breathing and Brook had to perform mouth-to-mouth respiration despite the presence of dirt,
blood, and vomit on the victim. The victim was
resuscitated successfully. This incident inspired
Brook to invent a device that could circumvent this
repulsive situation.7 Brook was not aware then that
Safar had already developed an S-shaped airway to
facilitate mouth-to-airway ventilation.8
The Brook airway (Fig) was introduced around
1959 and could be clipped onto the helmets of
miners. It consisted of an oral airway that helped to
displace the tongue and maintain a patent airway.
The flexible tube made ventilation feasible even
in awkward positions. The non-return valve was
designed such that exhaled air and contents of the
stomach could escape via a separate exit without
affecting the rescuer.9 To help popularise and teach
the use of his new airway, Brook developed a wooden
‘air passage demonstrator’ and a plastic mannequin
as training aids. He also produced a documentary
film ‘That They May Live’ to teach mouth-to-mouth
respiration. The Brook airway was simple and had
an additional advantage of being more flexible in
use. It was sold to health care providers and the
public in many countries in the 1960s and 1970s.
It appears that the Brook airway was not widely
used in Hong Kong, however, and was not standard
equipment for our local ambulance service. In time,
the widespread availability of resuscitation bags and
other supraglottic devices (eg the laryngeal mask)
made Brook’s airway obsolete.
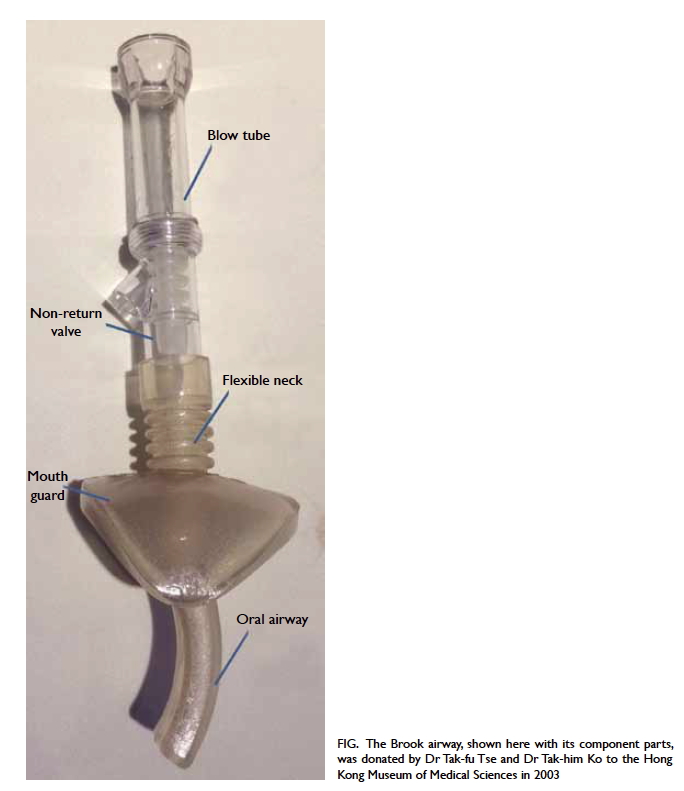
Figure. The Brook airway, shown here with its component parts, was donated by Dr Tak-fu Tse and Dr Tak-him Ko to the Hong Kong Museum of Medical Sciences in 2003
References
1. Tossach WA. A man dead in appearance recovered by distending the lungs with air. Med Essays Obs Soc Edinb 1744;part 2:605-8.
2. Baskett TF. Robert Woods (1865-1938): The rationale for mouth-to-mouth respiration. Resuscitation 2007;72:8-10. CrossRef
3. Elam JO, Brown ES, Elder JD Jr. Artificial respiration by mouth-to-mask method—A study of the respiratory gas exchange of paralyzed patients ventilated by operator’s expired air. N Engl J Med 1954;250:749-54. Crossref
4. Safar P. Ventilatory efficacy of mouth-to-mouth artificial respiration: airway obstruction during manual and mouth-to-mouth artificial respiration. J Am Med Assoc 1958;167:335-41. Crossref
5. Baskett PJ. Peter J. Safar, the early years 1924-1961, the birth of CPR. Resuscitation 2001;50:17-22. Crossref
6. Kouwenhoven WB, Jude JR, Knickerbocker GG. Closed-chest cardiac massage. JAMA 1960;173:1064-7. Crossref
7. Baskett TF. Resuscitation great. The Brook airway. Resuscitation 2006;71:6-9. Crossref
8. Safar P, McMahon M. Mouth-to-airway emergency artificial respiration. J Am Med Assoc 1958;166:1459-60. Crossref
9. Brook MH, Brook J, Wyant GM. Emergency resuscitation. Br Med J 1962;2:1564-6. Crossref