Hong Kong Med J 2016 Dec;22(6):623.e1–2
DOI: 10.12809/hkmj164889
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Posterior facet talocalcaneal non-osseous coalition: an uncommon but easily missed cause
of hindfoot pain
Arnold YH Tsang, MB, BS, FRCR;
YY Cheuk, FHKCR, FHKAM (Radiology);
Andrea WS Au-Yeung, FHKCR, FHKAM (Radiology)
Department of Diagnostic and Interventional Radiology, Kwong Wah
Hospital, Yaumatei, Hong Kong
Corresponding author: Dr Arnold YH Tsang (arnoldtsang@gmail.com)
 Full
paper in PDF
Full
paper in PDF
A 50-year-old female presented with chronic hindfoot
pain in July 2015. She was treated for plantar fasciitis
but the pain remained unresolved. Radiographs were
initially interpreted as degenerative changes only.
She was referred for further imaging. Review of the
radiographs showed an osseous prominence over the
posterosuperior aspect of the calcaneus, constituting
the abnormal shape of the posterior facet of the
subtalar joint with a humpback appearance on lateral
view (Fig 1a). Joint space of the medial posterior
facet was irregular and narrowed on Harris view
(Fig 1b). Magnetic resonance imaging (MRI) showed
the medial posterior facet of the subtalar joint to
be abnormally oblique on sagittal plane, and the
involved joint space was narrowed and irregular with
adjacent marrow oedema (Fig 2). No bony bridging
was seen. The middle facet was not involved. Included
tendons appeared unremarkable and plantar fascia
was not thickened. Features were suggestive of
fibrocartilaginous coalition at the medial aspect
of the posterior facet of the subtalar joint, also
referred to as posteromedial talocalcaneal coalition.
Computed tomography (CT) was also performed
for surgical planning, and demonstrated clearly the
irregular medial posterior facet, uninvolved middle
facet and lateral posterior facet (Fig 3).
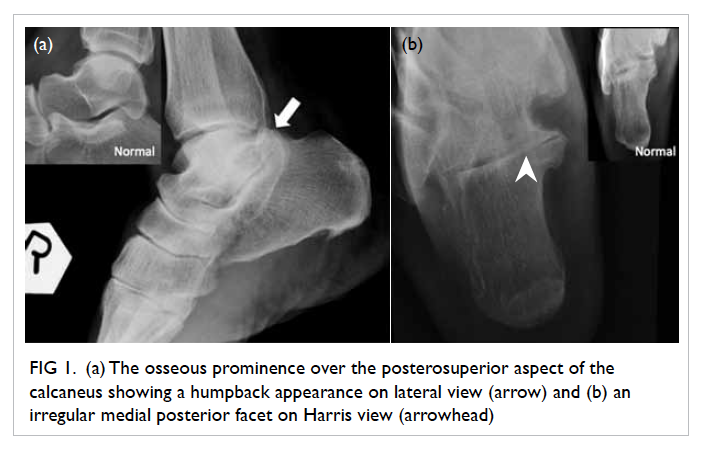
Figure 1. (a) The osseous prominence over the posterosuperior aspect of the calcaneus showing a humpback appearance on lateral view (arrow) and (b) an irregular medial posterior facet on Harris view (arrowhead)
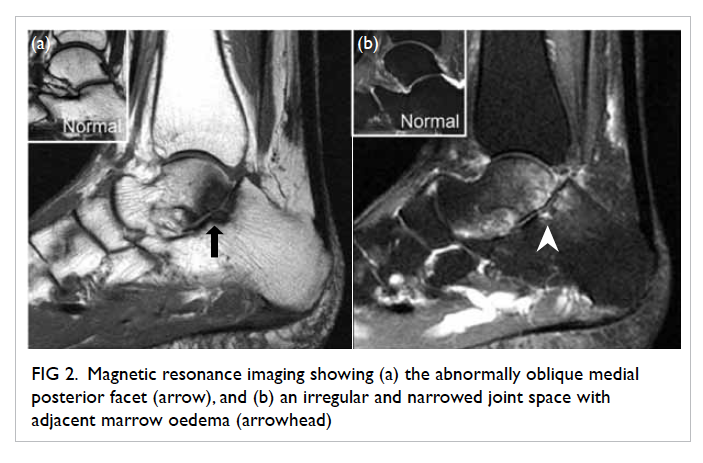
Figure 2. Magnetic resonance imaging showing (a) the abnormally oblique medial posterior facet (arrow), and (b) an irregular and narrowed joint space with adjacent marrow oedema (arrowhead)
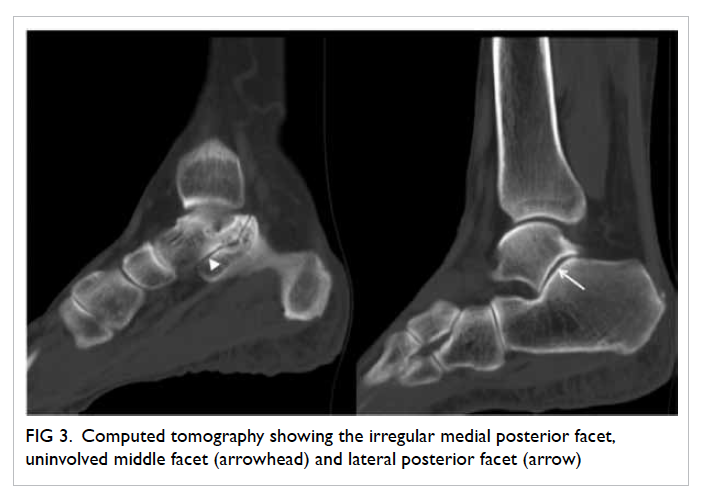
Figure 3. Computed tomography showing the irregular medial posterior facet, uninvolved middle facet (arrowhead) and lateral posterior facet (arrow)
Tarsal coalition can be osseous or
fibrocartilaginous. Calcaneonavicular and
talocalcaneal coalition accounts for 90% of hindfoot
coalition,1 2 of which 50% are bilateral.1 The talocalcaneal joint, also referred to as the subtalar
joint, consists of anterior, middle, and posterior
facets. Talocalcaneal coalition usually involves the
middle facet at the level of the sustentaculum tali.
The incidence of middle facet coalition is less than
1%.1 3 Involvement of the posterior facet is even
rarer, and is an easily missed cause of hindfoot pain.
Continuous C sign is the classic sign well described
for coalition over the middle facet. For posterior facet
coalition, the humpback sign as described above is the
radiographic finding to be recognised.1 3 4 The medial
aspect of the posterior facet is more commonly
involved, and Harris view can better demonstrate
the medial joint that will be irregular and narrowed
in non-osseous coalition. These findings are easily
misinterpreted as degenerative changes.
Cross-sectional imaging including CT and
MRI are valuable to confirm the diagnosis, define
the location and extent of the segmentation
anomaly, look for associated complications, and aid
preoperative planning. In particular, CT is useful in
determining the presence of any small bony bridging
and is important for surgical planning; MRI is able
to provide information about the degree of marrow
oedema that may correlate with level of pain. It
should be remembered that any unexplained marrow
oedema around the subtalar joint, which is an atypical
site for simple degenerative changes, should raise
the suspicion of coalition. Osseous coalition is less
likely to be missed on cross-sectional imaging as it
will appear grossly abnormal with bony fusion across
the involved facet (Fig 4). Potential complications of posterior facet coalition include peroneus
muscle spasms, sinus tarsi syndrome, tarsal tunnel
compression giving rise to a distended posterior
tibial vein, calcaneal stress fracture, and premature
osteoarthritis.1 4 Early recognition of non-osseous
posterior facet talocalcaneal coalition is important,
particularly in young patients, as surgical treatment
can reduce complications later in life.
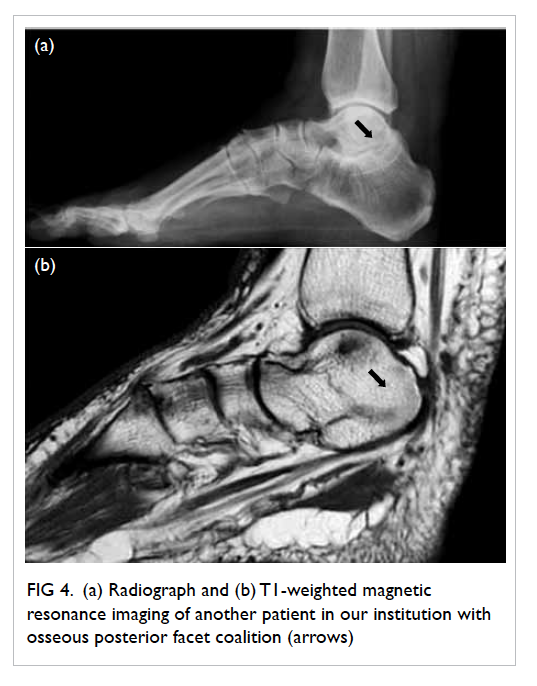
Figure 4. (a) Radiograph and (b) T1-weighted magnetic resonance imaging of another patient in our institution with osseous posterior facet coalition (arrows)
References
1. Staser J, Karmazyn B, Lubicky J. Radiographic diagnosis
of posterior facet talocalcaneal coalition. Pediatr Radiol
2007;37:79-81. Crossref
2. Newman JS, Newberg AH. Congenital tarsal coalition:
multimodality evaluation with emphasis on CT and MR
imaging. Radiographics 2000;20:321-32. Crossref
3. McNally EG. Posteromedial subtalar coalition: imaging
appearances in three cases. Skeletal Radiol 1999;28:691-5. Crossref
4. Moe DC, Choi JJ, Davis KW. Posterior subtalar facet
coalition with calcaneal stress fracture. AJR Am J
Roentgenol 2006;186:259-64. Crossref