Hong Kong Med J 2016 Aug;22(4):399.e4–5
DOI: 10.12809/hkmj164864
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Crowned dens syndrome: an uncommon cause of cord compression
Cindy SY Fung, MB, ChB, FRCR;
Godfrey KF Tam, FRCR, FHKCR
Department of Radiology, North District Hospital, Sheung Shui, Hong Kong
Corresponding author: Dr Cindy SY Fung (sycindy@gmail.com)
 Full
paper in PDF
Full
paper in PDF
A 65-year-old man presented to our hospital in
June 2015 with a 2-week history of neck pain and
progressive weakness in four limbs. There was no
recent trauma history. He had a history of cervical
myelopathy with decompression performed in
2011. On physical examination, an old scar on his
neck was unremarkable with no signs of infection.
Neurological examination revealed generalised
weakness in all four limbs, more marked in bilateral
upper limbs. All limbs were hypertonic with
hyperreflexia. There was no sensory loss. His C-reactive
protein level was elevated to 39.6 mg/L,
white blood cell count was also elevated to 14.8 x 109 /L. His cervical radiograph showed indistinct
dens (Fig 1). No abnormal soft tissue thickening was seen. Screws of the previous posterior cervical
decompression were in-situ. Computed tomography
was performed and revealed erosion of the dens and
some mildly hyperdense periodontoid soft tissue (Fig 2). Further study with magnetic resonance imaging
showed T1 intermediate, T2 heterogeneously
hypointense periodontoid soft tissue with patchy
enhancement (Fig 3). The cervicomedullary junction was moderately compressed with internal T2
hyperintense cord signal, signifying cord oedema
or myelomalacia. Radiograph of other joints found
chondrocalcinosis in the triangular fibrocartilage of
the right wrist, which is also a common manifestation
of calcium pyrophosphate dihydrate (CPPD) crystal
deposition disease (Fig 4). Overall features were compatible with crowned dens syndrome.
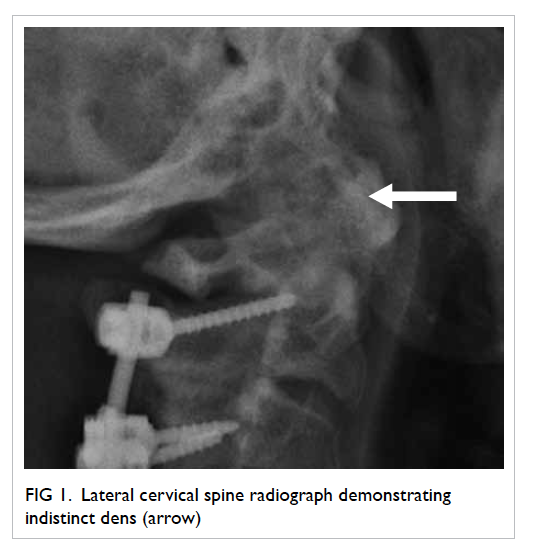
Figure 1. Lateral cervical spine radiograph demonstrating indistinct dens (arrow)
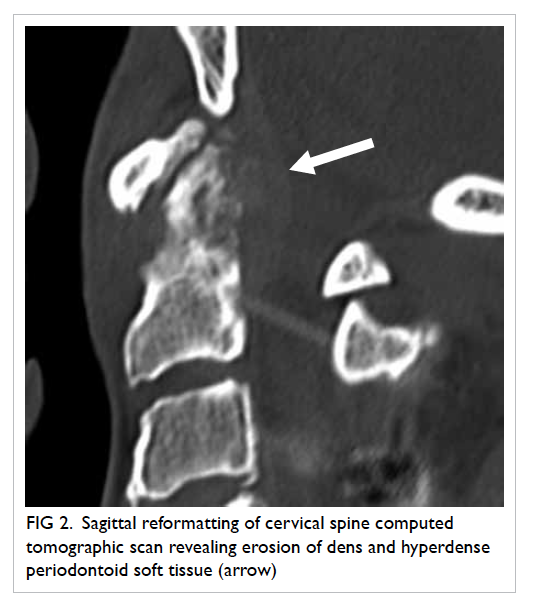
Figure 2. Sagittal reformatting of cervical spine computed tomographic scan revealing erosion of dens and hyperdense periodontoid soft tissue (arrow)
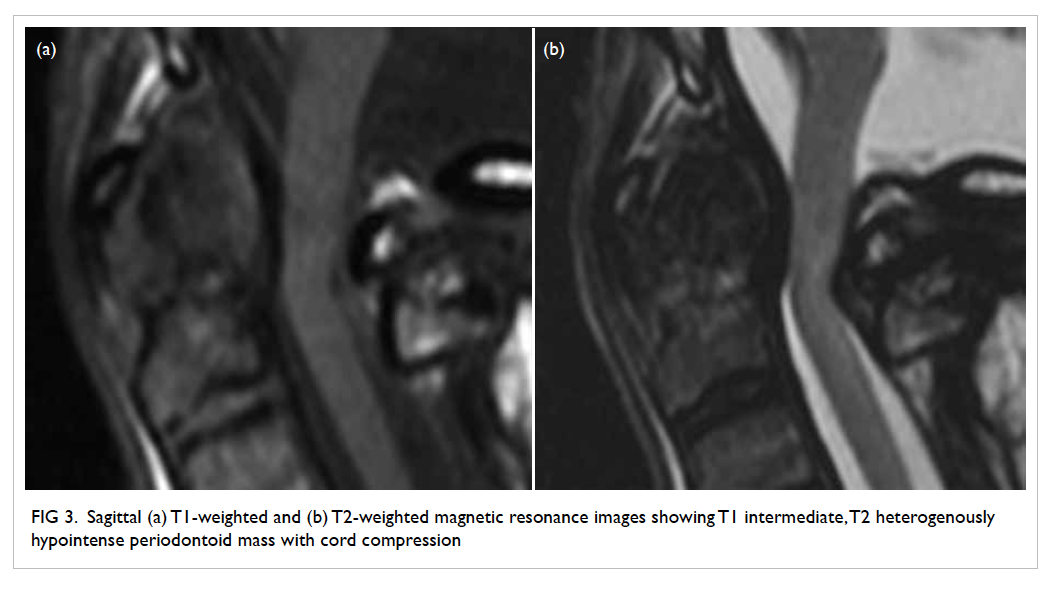
Figure 3. Sagittal (a) T1-weighted and (b) T2-weighted magnetic resonance images showing T1 intermediate, T2 heterogenously hypointense periodontoid mass with cord compression

Figure 4. Radiograph of other joints found chondrocalcinosis of the triangular fibrocartilage in the right wrist, compatible with calcium pyrophosphate dihydrate crystal deposition disease
Crowned dens syndrome was first described
by Bouvet et al in 1985.1 It is a rare entity that
presents clinically with severe upper neck pain and
radiologically a crown-like density surrounding the
odontoid process caused by deposition of CPPD
crystals, which is now more commonly described,
or hydroxyapatite (HA).1 It is more common in
elderly patients with no history of trauma. Increased
inflammatory indicators, such as an elevated C-reactive
protein, are usually seen.2 Diagnosis is not
easy as crowned dens syndrome can mimic a wide
range of diseases such as meningitis, osteomyelitis,
degenerative cervical spine disease, ankylosing
spondylitis, gout, rheumatoid arthritis, temporal
arteritis, metastatic bone disease, and spinal
tumours.3 Computed tomography is the gold
standard for identifying crowned dens syndrome, as
it is able to depict the shape and site of calcification
and any bone erosions. Radiography of other joints
(wrist, knee, pubic symphysis) may help to ascertain
whether the disease is due to CPPD or HA crystals,
and is therefore recommended for routine patient
management. Magnetic resonance imaging is
indicated for the study of neurological complications
as in our patient.4 Prednisolone and non-steroidal
anti-inflammatory drugs in combination are the
recommended treatment for symptom relief.2
Crowned dens syndrome is an under-recognised
disease. Familiarity with the clinical
and radiological features will help doctors provide
prompt and effective treatment.
References
1. Bouvet JP, le Parc JM, Michalski B, Benlahrache C, Auquier
L. Acute neck pain due to calcifications surrounding the
odontoid process: the crowned dens syndrome. Arthritis
Rheum 1985;28:1417-20. Crossref
2. Goto S, Umehara J, Aizawa T, Kokubun S. Crowned dens
syndrome. J Bone Joint Surg Am 2007;89:2732-6. Crossref
3. Wu DW, Reginato AJ, Torriani M, Robinson DR, Reginato
AM. The crowned dens syndrome as a cause of neck
pain: report of two new cases and review of the literature.
Arthritis Rheum 2005;53:133-7. Crossref
4. Scutellari PN, Galeotti R, Leprotti S, Ridolfi M, Franciosi
R, Antinolfi G. The crowned dens syndrome. Evaluation
with CT imaging. Radio Med 2007;112:195-207. Crossref