DOI: 10.12809/hkmj144411
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
CASE REPORT
Trampoline-related injuries in Hong Kong
MY Cheung, MB, BS; CL Lai, MB, BS; Wilson HY Lam, MB, BS; James SK Lau, BSc, MB, BS; Aaron KH Lee, MB, ChB; Gabrielle G Yuen, MB, BS; YK Chan, FRCS, FHKAM (Orthopaedic Surgery); WL Tsang, FRCS, FHKAM (Orthopaedic Surgery)
Department of Orthopaedics and Traumatology, Pamela Youde Nethersole Eastern Hospital, Chai Wan, Hong Kong
Corresponding author: Dr James SK Lau (jameslau@gmail.com)
 Full
paper in PDF
Full
paper in PDF
Case reports
The following three cases highlight the potential
serious consequences of trampolining.
Case 1: Lisfranc fracture
A 27-year-old woman with good past health was
admitted with left foot pain and swelling in July
2014. She fell with axial loading on an inverted and
plantar-flexed left foot while trampolining. Physical
examination showed bruising on the dorsum of her
left foot with tenderness over the base of the first and
second metatarsals. Range of movement was limited
by pain. Subsequent X-ray showed widening of the
Lisfranc joint with base avulsion (Fig a). Lisfranc
fracture was diagnosed. Open reduction with screw
and K-wire fixation were performed and a resting
ankle-foot orthosis was given. On follow-up 2 weeks
after surgery, sensation and circulation in the toes
were good. Range of movement was still limited
by pain, however. She was encouraged to move her
ankle and toes, and to mobilise with heel-walking at
6 weeks postoperatively.

Figure. Images of the case illustrations
(a) X-ray of the left foot (dorsoplantar view) of patient 1 showing widening of Lisfranc joint (arrow). (b) Computed tomography of the spine (reconstructed sagittal view) of patient 2 demonstrating two-column fractures of T12 and L1 (arrows). (c) X-ray of the left ankle (lateral view) of patient 3 illustrating posterior talus dislocation (arrow)
Case 2: vertebral fracture
A 25-year-old swimming instructor with good past
health was admitted for thoracolumbar back pain
after jumping and falling from 1 metre while trampolining in August 2014.
He landed on his upper back with his body flexed
on a trampoline. On examination, there was local
tenderness at the thoracolumbar junction. His power
and sensation across L2 to S1 were normal, reflexes
were present, and anal sensation and tone were
intact. Lumbosacral spine X-ray showed collapsed
T12 and L1 with local kyphosis of 25°. Computed
tomographic scan was performed subsequently,
detailing a two-column fracture of T12 and L1 with
anterior wedging of 20% (Fig b). He was put on a rigid
thoracolumbar orthosis for 8 weeks and prescribed
analgesics. Close monitoring for further collapse was
warranted. During follow-up, he had no complaints
of pain or neurological symptoms. Follow-up X-ray
of the lumbosacral spine was static.
Case 3: ankle dislocation
A 22-year-old woman with good past health was
admitted with left ankle pain and deformity after
landing on a trampoline with plantar flexion and
ankle inversion in August 2014. Physical examination
revealed a deformed left ankle joint in medial
rotation and plantar flexion. There was bruising over
the left foot dorsum and marked tenderness over the
whole ankle joint line. She could move her toes only
slightly. Distal circulation was intact, but sensation
was reduced over her left foot and toes. X-ray of the
left ankle showed posterior talus dislocation without
definite fracture (Fig c). Closed reduction was
performed under sedation and a short leg slab was
applied. Post-reduction X-ray showed a congruent
ankle joint. Computed tomography showed no
fracture. Magnetic resonance imaging of the left
ankle showed small cortical fractures at the medial
body of talus and posterior aspect of distal talus,
complete tear of the calcaneofibular ligament and
anterior talofibular ligament, and a partial thickness
tear of the deep deltoid ligament. Immobilisation
with a short leg cast is planned after oedema has
subsided.
Discussion
In Hong Kong, trampolining was once a part of
school physical education classes since it improves
motor control and increases physical activity.1
However, following a trampoline incident in
1991 that resulted in quadriplegia,2 its popularity
dwindled. Since the opening of the first trampoline
park in Hong Kong in late July 2014,3 an increase in
the number of trampoline-related injuries requiring
admission to our department has been noted. Eight
trampoline-related admissions were observed in
less than 2 months. It has been estimated that the
incidence of injuries that required admission to our
unit was 1.9 per 10 000.4 The reasons of admission
included Lisfranc fracture, vertebral fracture,
ankle dislocation, anterior cruciate ligament tear
of the knee, and neck and back sprains (Table).
All patients were previously healthy but had no
trampolining experience when they attended the
indoor trampoline park for recreation and injured
themselves while landing on a trampoline mat.
Physicians and the general public need to be aware
that trampolining can result in significant injuries,
leading to acute hospital admission or even early
surgical attention.
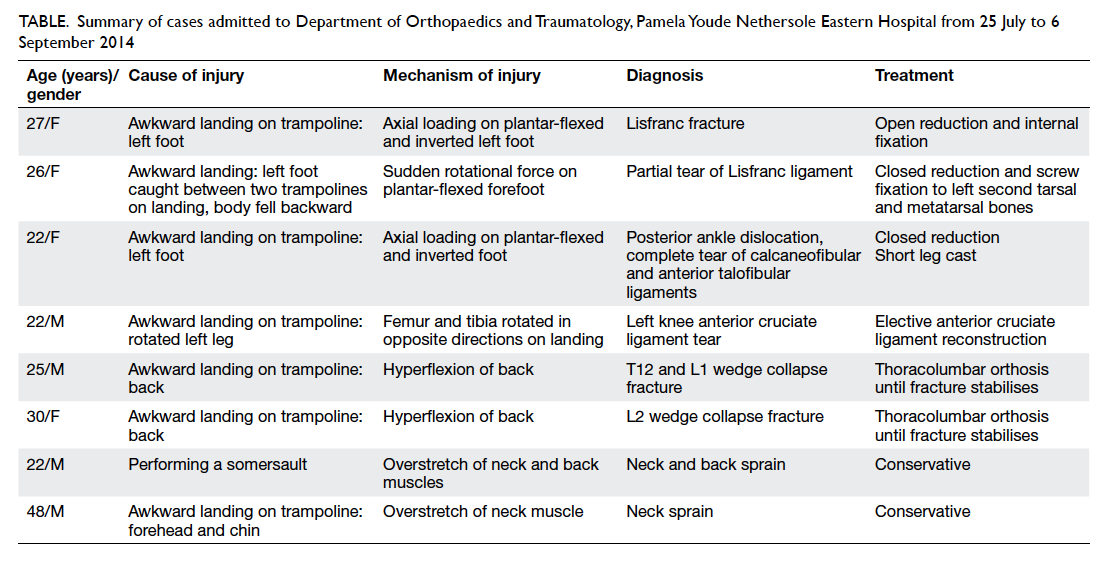
Table. Summary of cases admitted to Department of Orthopaedics and Traumatology, Pamela Youde Nethersole Eastern Hospital from 25 July to 6 September 2014
Literature review
In a New Zealand study, most trampoline injuries
occurred on home trampolines.5 With its limited
space, home trampolining is not popular in Hong
Kong, thus there is a lack of local studies. Nonetheless
since the recent opening of a trampoline park in
our cluster, the awareness of trampoline-related
injuries has risen rapidly. In less than 2 months,
eight patients were admitted for trampoline-related
injuries. Their age ranged from 22 to 48 years, with
seven aged between 22 and 30 years. In overseas
studies, the highest incidence of injury occurred in
patients under 20 years of age.5 6 This is related to accessibility to home trampolines.
Nysted and Drogset1 evaluated a total of 551
injuries, among which 292 cases were secondary to
awkward landing on the trampoline1 in comparison
with seven out of eight cases observed locally. The
second and third most common mechanism of
injury was falling off the trampoline and collision
with another person, respectively.1 Falling off the
trampoline is not possible in our setting since
there are multiple interconnected trampolines
that are levelled with a padded ground. The fourth
commonly reported injury was caused by performing
a somersault (11%)1 on the trampoline which was
the cause of injury in our eighth patient. In another
study by Alexander et al,7 a similar trend is seen. A
majority of injuries (42%) were due to landing badly
on the trampoline. Injuries from the frame/springs,
presence of multiple jumpers, and getting on/off constituted 19%, 10% and 2% of all trampoline
injuries, respectively. In short, serious injuries can
happen even when landing on a soft surface such
as a trampoline mat where participants may be less
cautious.
In our report, there was a lack of injuries
involving the upper extremities, contrary to the
findings of overseas studies. This could be skewed
by the small sample size as well as the nature of
trampolining; untrained adults tend to be more
conservative and land axially on their feet. Hence the
majority of our cases involved the lower extremities
(50%), and is congruent with the findings of Hume
et al5 and Nysted and Drogset1 (46% and 45%, respectively). Another important point to note is
that injuries involving the spine are not uncommon
(25%).
Regarding the types of injury, fractures
constituted a significant proportion of injuries in the
studies of Nysted and Drogset1 and Chalmers et al8 (36% and 68%, respectively), and was also the case
in our study (37.5%). A small proportion of local
injuries were dislocation, which is observed in the
same studies.1 8
Safety measures
In addition to regular maintenance and a readily
available first-aid kit, a number of measures can
be taken that may lower the injury rates. Most
importantly, participants should be verbally briefed
by the facility provider about the risks and dangers of
trampoline use.9 For example, only one participant
should be on a trampoline mat at any given time.9
Black and Amadeo10 emphasised the importance
of multiple jumpers as a risk factor for injuries due
to the elastic recoil generated by a larger person
jumping on the mat.
In order to familiarise participants with the
elasticity of a trampoline, trampolines of lower
elasticity should be provided for warm-up. This is
a common practice in formal training,11 and may
reduce the chance of awkward landing due to motor
incoordination. Another suggestion is to restrict
beginners from performing complex movements
such as somersaults and flips.9 To achieve this, the
provider may provide a separate area for advanced
participants. It is important to note that padding to
cover frames has not been shown to reduce injuries.7
Injury rates should be monitored8 closely by the
provider so that the effectiveness of safety measures
can be evaluated.
Limitations and suggestions
Injuries that did not require hospital admission were
not included, such as those in patients who presented
to general practitioners or who were discharged from
the emergency department. Furthermore, this report
can only include cases that occurred up to the time
of writing. This may underestimate the problem and
lead to inaccurate interpretation. It is also difficult
to draw comparisons with epidemiological data
from other countries where the majority of injuries
arise from home trampoline use and not from
trampoline parks. Lastly, although trampolining
may be perceived as a dangerous physical activity,
this may not be the case; the risk of injury is not high
compared with other physical activities.
Acknowledgement
We thank Dr Siu-ho Wan for encouragement,
guidance, and assistance throughout the preparation
of the case reports.
References
1. Nysted M, Drogset JO. Trampoline injuries. Br J Sports
Med 2006;40:984-7. Crossref
2. Tang SP. I want euthanasia [In Chinese]. Hong Kong: Joint
Publishing (HK) Co Ltd; 2007.
3. South China Morning Post. Hong Kong’s first trampoline
park, Ryze, is bound to be fun. Available from: http://yp.scmp.com/news/sports/article/90339/hong-kongs-first-trampoline-park-ryze-bound-be-fun. Accessed 4 Sep 2014.
4. South China Morning Post. Trampoline centre Ryze proves
a summer hit with Hong Kong youth. Available from: http://www.scmp.com/news/hong-kong/article/1565201/trampoline-centre-ryze-proves-summer-hit-hong-kong-youth.
Accessed 26 Feb 2014.
5. Hume PA, Chalmers DJ, Wilson BD. Trampoline injury
in New Zealand: emergency care. Br J Sports Med
1996;30:327-30. Crossref
6. Hammer A, Schwartzbach AL, Paulev PE. Trampoline
training injuries—one hundred and ninety-five cases. Br J
Sports Med 1981;15:151-8. Crossref
7. Alexander K, Eager D, Scarrott C, Sushinsky G.
Effectiveness of pads and enclosures as safety interventions
on consumer trampolines. Inj Prev 2010;16:185-9. Crossref
8. Chalmers DJ, Hume PA, Wilson BD. Trampolines in New
Zealand: a decade of injuries. Br J Sports Med 1994;28:234-8. Crossref
9. Council on Sports Medicine and Fitness, American
Academy of Pediatrics, Briskin S, LaBotz M. Trampoline
safety in childhood and adolescence. Pediatrics
2012;130:774-9. Crossref
10. Black BG, Amadeo R. Orthopedic injuries associated
with backyard trampoline use in children. Can J Surg
2003;46:199-201.
11. USA Gymnastics. Basic trampoline—the beginning
steps. Available from: https://usagym.org/pages/home/publications/technique/2000/3/basictrampoline.pdf.
Accessed 8 Sep 2014.