Hong Kong Med J 2015 Jun;21(3):237–42 | Epub 8 May 2015
DOI: 10.12809/hkmj144344
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
ORIGINAL ARTICLE
Mechanism and epidemiology of paediatric finger injuries at Prince of Wales Hospital in
Hong Kong
WH Liu, MB, BS; Johann Lok, MB, ChB; MS Lau, MB, ChB; YW Hung, FHKCOS, FHKAM (Orthopaedic Surgery); Clara WY Wong, FHKCOS, FHKAM (Orthopaedic Surgery); WL Tse, FHKCOS, FHKAM (Orthopaedic Surgery);
PC Ho, FHKCOS, FHKAM (Orthopaedic Surgery)
Department of Orthopaedics and Traumatology, Prince of Wales Hospital,
The Chinese University of Hong Kong, Shatin, Hong Kong
Corresponding author: Dr WH Liu (liuwinghong@yahoo.com.hk)
This paper was presented at the 27th Annual Congress of the Hong Kong
Society for Surgery of the Hand, 15-16 March 2014, Hong Kong.
 Full
paper in PDF
Full
paper in PDF
Abstract
Objectives: To determine the mechanism and
epidemiology of paediatric finger injuries in Hong
Kong during 2003-2005 and 2010-2012.
Design: Comparison of two case series.
Setting: University-affiliated teaching hospital, Hong Kong.
Patients: This was a retrospective study of two cohorts of
children (age, 0 to 16 years) admitted to Prince of
Wales Hospital with finger injuries during two 3-year
periods. Comparisons were made between the
two groups for age, involved finger(s), mechanism
of injury, treatment, and outcome. Telephone
interviews were conducted for parents of children
who sustained a crushing injury of finger(s) by door.
Results: A total of 137 children (group A) were
admitted from 1 January 2003 to 31 December
2005, and 109 children (group B) were admitted
from 1 January 2010 to 31 December 2012. Overall,
the mechanisms and epidemiology of paediatric
finger injuries were similar between groups A and
B. Most finger injuries occurred in children younger
than 5 years (group A, 56%; group B, 76%) and in
their home (group A, 67%; group B, 69%). The most
common mechanism was crushing injury of finger by
door (group A, 33%; group B, 41%) on the hinge side
(group A, 63%; group B, 64%). The right hand was
most commonly involved. The door was often closed
by another child (group A, 37%; group B, 23%) and
the injury often occurred in the presence of adults
(group A, 60%; group B, 56%). Nailbed injury was the
commonest type of injury (group A, 31%; group B,
39%). Fractures occurred in 24% and 23% in groups
A and B, respectively. Traumatic finger amputation
requiring replantation or revascularisation occurred
in 12% and 10% in groups A and B, respectively.
Conclusions: Crushing injury of finger by door
is the most common mechanism of injury among
younger children and accounts for a large number
of hospital admissions. Serious injuries, such as
amputations leading to considerable morbidity,
can result. Crushing injury of finger by door occurs
even in the presence of adults. There has been no
significant decrease in the number of crushing
injuries of finger by door in the 5 years between the
two studies despite easily available and affordable
preventive measures. It is the authors’ view that
measures aimed at promoting public awareness and
education, and safety precautions are needed.
New knowledge added by this
study
- Similar to other countries, crushing injury of finger by door was the most common cause of paediatric finger injuries in Hong Kong.
- Although many preventive measures are available and easily accessible at low cost, there were no significant differences in injury mechanism and epidemiology between 2003-2005 and 2010-2012.
- Paediatric crushing injury of finger by door can occur even in the presence of adults. Reinforcement of public education on the use of safety measures, including door modification and precautions in the home, should be conducted to prevent such injuries.
Introduction
Injuries to the hand and fingers are extremely
common in children, yet they can have a significant impact on a child’s growth and development. Fingers
are used to explore surroundings and perform daily
activities such as playing, eating, and homework.
Restricting children from these activities due to
injuries can have immediate short- and long-term
detrimental effects on the function of the hand,
psychological wellbeing, and quality of life of the
children. A 10-year review on the psychological
impact on children and adolescents with finger or
hand injuries noted that “Hand injuries are common
and loss of a dominant hand or opposition is most
important [sic]. Self-esteem and skill are associated
with hand sensation, appearance, and functions.”1
Studies by Al-Anazi2 and Doraiswamy3 have identified crushing injury of finger(s) by door as the
main cause of finger injuries in children. However,
there has been no local study to identify the main
cause of finger injuries in Hong Kong. In 2007,
Lau and Ho presented data on the epidemiology of
childhood finger injuries (unpublished data; Lau M,
Ho PC. 20th Annual Congress of the Hong Kong
Society for Surgery of the Hand, Hong Kong, 2007)
that supported the findings in other cities. Similar
to Al-Anazi2 and Doraiswamy,3 Lau and Ho found
that crushing injury of finger by door was the most
common cause of paediatric finger injuries from
2003 to 2005, and recommended various preventive
measures.
The present study aimed to compare the
previous set of data from 2003 to 2005 reported by
Lau and Ho with more recent data obtained from
2010 to 2012. By comparing the epidemiology and
mechanisms of finger injuries among local Hong
Kong children, we aimed to determine whether there
have been any significant changes over the past 5
years.
Methods
Data of patients admitted to Prince of Wales
Hospital from 1 January 2003 to 31 December 2005
(group A) and from 1 January 2010 to 31 December
2012 (group B) were retrieved using the Clinical
Data Analysis and Reporting System (CDARS) of the
Hospital Authority’s Clinical Management System.
Children aged 0 to 16 years, and with at least one
of the International Classification of Diseases, 9th
Revision, Clinical Modification (ICD-9-CM) codes
listed in the Box among the top three diagnoses were
included in the analysis.
Box. CDARS case finding list of Prince of Wales Hospital
Discharge summaries of all patients were
reviewed to identify the mechanisms of finger
injuries. For children in whom the mechanism was
not immediately discernable from the discharge
summary, further clarifications were obtained by
telephone interviews with the child’s parents, which
were conducted in 2006 for group A and in 2013 for
group B. For children in whom crushing injury of
finger(s) were due to closing doors, additional data
were collected by telephone interviews with their
parents using a specifically designed questionnaire
(Fig 1).
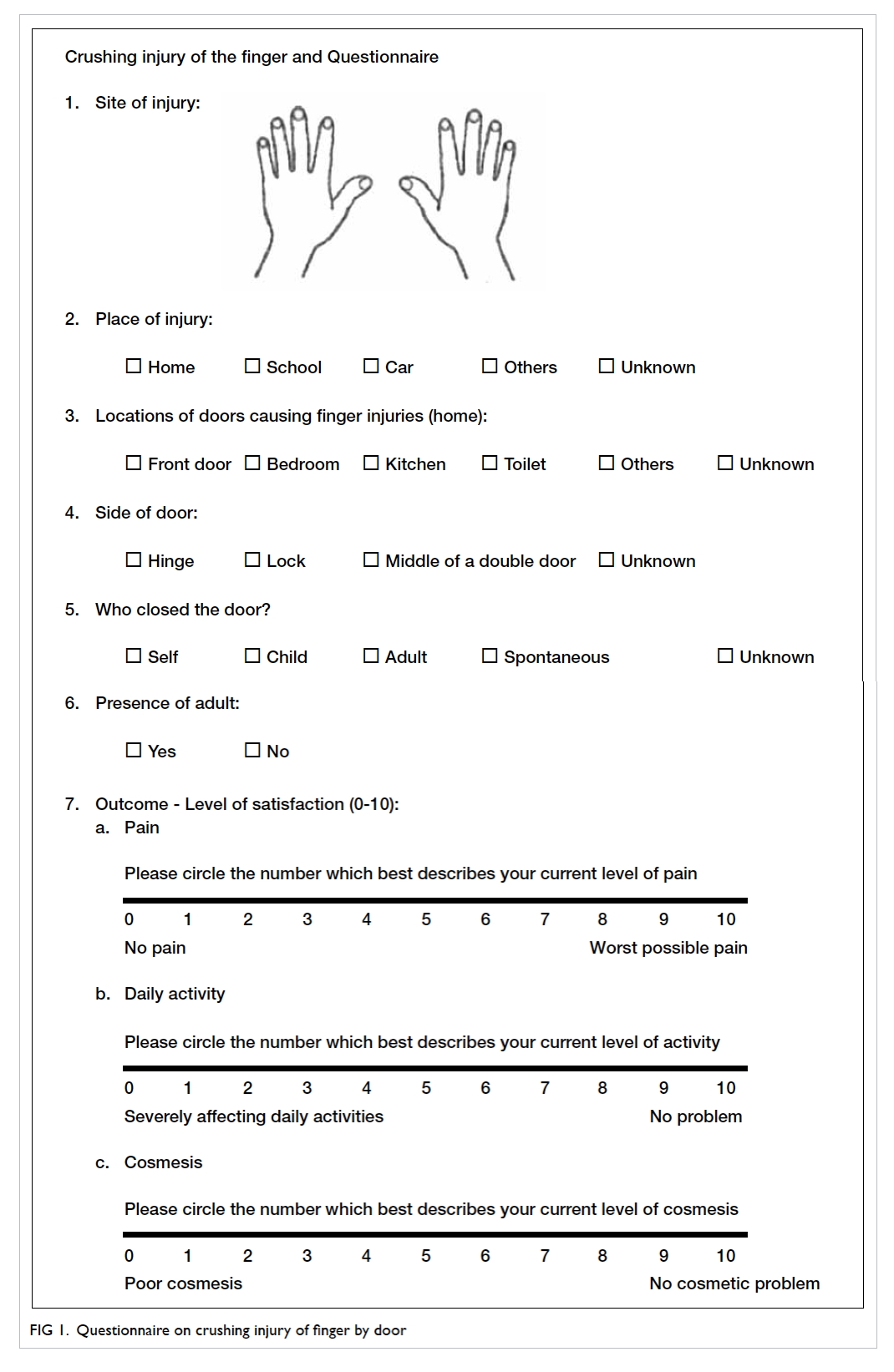
Figure 1. Questionnaire on crushing injury of finger by door
Results
Group A consisted of 140 children who presented
with finger injury to Prince of Wales Hospital from
1 January 2003 to 31 December 2005. Three children
from this group were excluded due to coding error.
Group B comprised 109 children who presented
from 1 January 2010 to 31 December 2012. No
children from this group were excluded.
In both groups, crushing injury of finger by
door was the most common cause of injury—45
(33%) in group A and 45 (41%) in group B—followed
by sports injury, cut, and slip and fall (Table 1).
Among children with crushing injury of finger by
door, younger children were the most commonly
injured (Fig 2a). The male-to-female ratio was 1:1.25
in group A and 1.37:1 in group B.
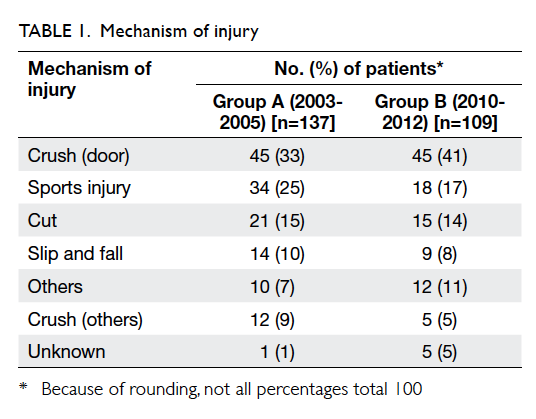
Table 1. Mechanism of injury
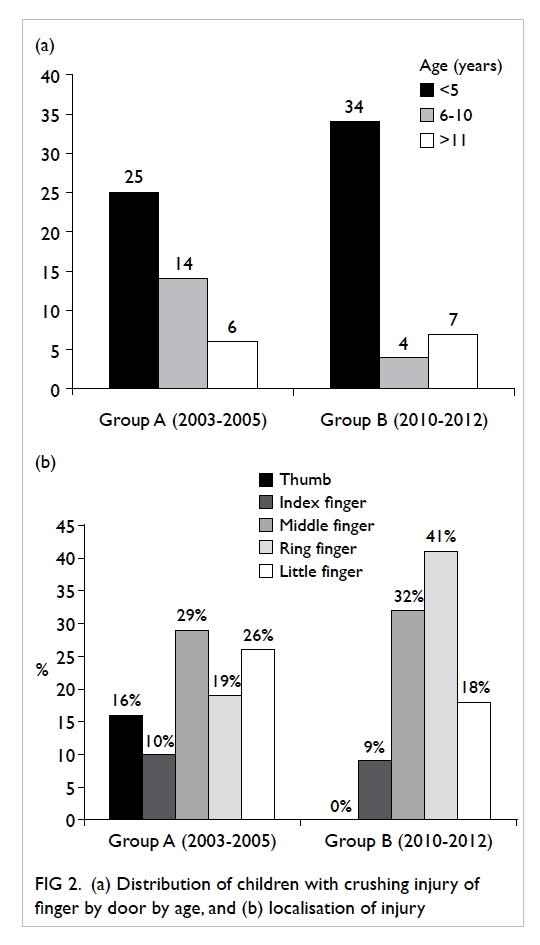
Figure 2. (a) Distribution of children with crushing injury of finger by door by age, and (b) localisation of injury
In the telephone interviews conducted with the
parents of the 45 children who had crushing injury
of finger by door, parents of two children in group A
and six children in group B could not be contacted.
Overall, all the parameters measured were similar
between the periods 2003-2005 and 2010-2012.
In both groups, most of the fingers involved were
from the right hand, with the middle, ring, and little
fingers being more commonly affected than the
other fingers (Fig 2b).
Most of the injuries occurred at home—29
(67%) in group A and 27 (69%) in group B. At home,
fingers were most frequently crushed at the hinge
side of the door—27 (63%) in group A and 25 (64%)
in group B—followed by the lock side and the middle
of a double door. The doors were frequently closed
by another child—16 (37%) in group A and 9 (23%) in
group B and, in more than half of the cases, occurred
even in the presence of adults—26 (60%) in group A
and 22 (56%) in group B (Table 2).
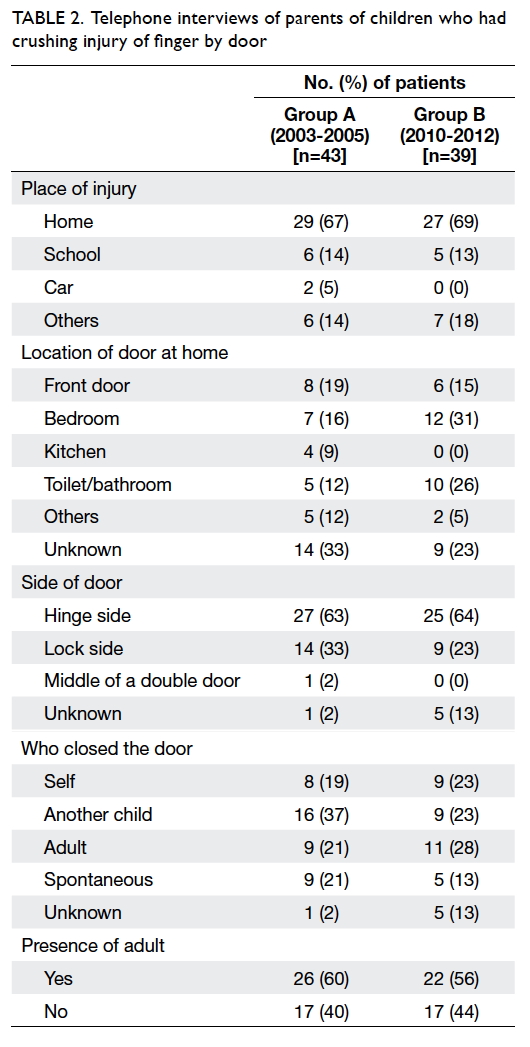
Table 2. Telephone interviews of parents of children who had crushing injury of finger by door
The types of injury and their relative
frequencies were compared between the groups
(Table 3). Among the more common injuries were: nailbed injury—22 (31%) in group A and 22 (39%) in
group B; fracture—17 (24%) in group A and 13 (23%)
in group B; and laceration—17 (24%) in group A and
11 (20%) in group B. Most of the children in both
group A (31 [72%]) and group B (30 [77%]) required
operation. Among the 31 operations in group A, 21
(68%) were performed under general anaesthesia. By
contrast, only 12 (40%) of the 30 operations in group
B involved general anaesthesia.
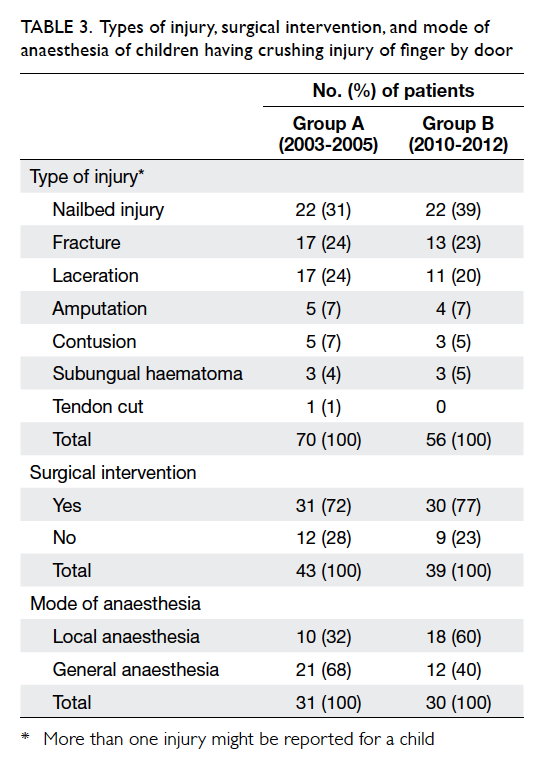
Table 3. Types of injury, surgical intervention, and mode of anaesthesia of children having crushing injury of finger by door
Clinical outcomes were assessed when the
telephone interviews were conducted, ie, in 2006
for group A and in 2013 for group B. Most children
had a good recovery following treatment. Overall,
42 (98%) of children in group A and 37 (94%) of
children in group B reported no pain. Only minor
cosmetic problems prevailed in most children, with
34 (79%) in group A and 35 (89%) in group B rating
their current level of cosmesis over 7 out of 10 (score
10 = no cosmetic problem). The injuries had minimal
adverse effects for most children, with 42 (98%) in
group A and 39 (100%) in group B rated their daily
activities with a score over 8 (score 10 = no problem)
[Fig 3].
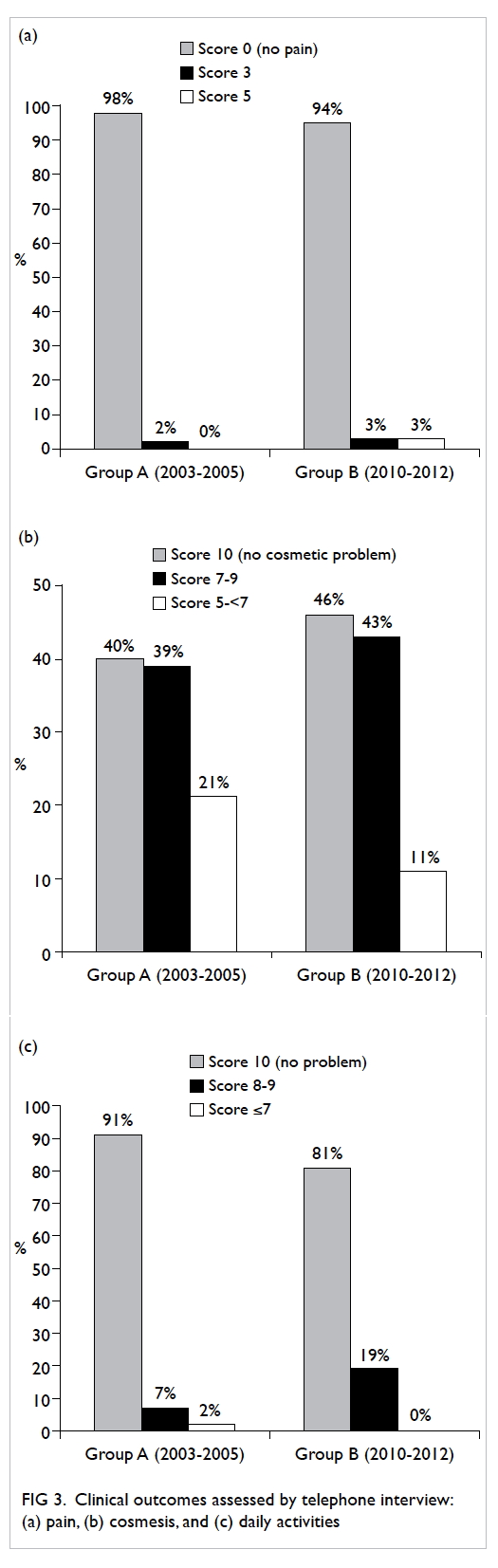
Figure 3. Clinical outcomes assessed by telephone interview: (a) pain, (b) cosmesis, and (c) daily activities
However, five (12%) children in group A and
four (10%) children in group B had crushing injury
of finger by door resulting in finger amputation.
Altogether seven children in groups A and B
received replantation or revascularisation, one child
underwent open reduction and fixation only, and
one had a failed replantation due to failure to locate
the arteries intra-operatively.
In group A, one child developed thrombosis
following replantation of the right ring finger,
requiring a subsequent revascularisation procedure
3 days later. This was complicated by hooknail
deformity 1 year post-replantation and was
subsequently treated by further reconstructive
procedures. The levels of satisfaction in terms of
appearance and daily function at final follow-up
were rated 5 and 3 (out of 10, with 10 means no
cosmetic problem and no problem in daily activities),
respectively.
Discussion
Crushing injury of finger by door is common. The
true incidence of this type of injury is likely to be
higher, as our data were limited to public hospitals
so relied on the correct entry of ICD-9-CM codes
into the CDARS. Data from the accident and
emergency department and private practitioners
were not analysed. Furthermore, many minor
injuries might have been managed at home and not
reported.
Crushing injury of finger by door is not just
a local problem. Studies from Saudi Arabia and
Glasgow showed that this type of injury accounted
for most childhood fingertip injuries in these areas.2 3 These injuries consistently occurred at home, with
the involved finger being frequently crushed at the
hinge side of doors. Younger children were mostly
affected. The similarity in epidemiology between
the overseas data and our local data can help with
recommendations for suitable door safety devices.
In this study, we identified that crushing injury
by door was the major cause of paediatric finger
injuries leading to hospital admission in both 2003-2005 and 2010-2012. Although most children were
satisfied with the level of pain, cosmesis, and daily
function of the injured digit at their final follow-up
after treatment, serious injuries involving fractures
and amputations occurred in a minority of patients.
In addition to the surgical intervention and long-term
hospitalisation required, these injuries could
further lead to detrimental effects on the children’s
growth and development.
Our study showed the presence of adults did
not reduce the rate of these accidents, since most
occurred even in the presence of an adult. This
highlights the need for other preventative measures.
Many types of safety devices are easily
available and affordable in Hong Kong. As the hinge
side of doors is the most common side for fingers
to be crushed, finger guard devices can be installed
to prevent fingers being trapped in the opposing
surfaces. Triangular-shaped rubbers, plastic or
wooden stoppers can be inserted at the bottom of
a door to prevent spontaneous closure. Magnets
applied to the back of a door and its opposing wall
surface present another equally effective and simple
method of preventing unintended door closures.
Dampers can be set up to reduce the speed of closing
doors, thereby decreasing the force exerted on
trapped fingers. The use of automatic doors should
be avoided.
Yet, despite the easy availability and
accessibility of these safety devices, there has been
no significant change or improvement in terms of
incidence and morbidity of children with crushing
injury of fingers by door admitted to Prince of Wales
Hospital in the 5-year period between 2003-2005
and 2010-2012. Thus, we should promote public
awareness about this type of injury and provide
more educational programmes on safety precautions
in order to reduce the incidence of crushing injury
of finger by door.
Conclusions
Crushing injury of finger by door accounts for the
most common cause of paediatric finger injury
requiring hospitalisation in Hong Kong. These
injuries frequently result in hospital admission and
surgical intervention, with considerable morbidity
and high treatment cost. Crushing injury of finger by
door occurs even in the presence of adults. Despite
the easily available and affordable preventative
measures in Hong Kong, our comparison revealed
no significant difference in the incidence, nature, and
severity of these domestic injuries between the years
2003-2005 and 2010-2012. Thus, it is our view that
more effort should be invested into raising public
awareness and education about these preventable
injuries and to promote prevention measures.
References
1. Stoddard F, Saxe G. Ten-year research review of physical
injuries. J Am Acad Child Adolesc Psychiatry 2001;40:1128-45. Crossref
2. Al-Anazi AF. Fingertip injuries in paediatric patients—experiences at an emergency centre in Saudi Arabia. J Pak Med Assoc 2013;63:675-9.
3. Doraiswamy NV. Childhood finger injuries and safeguards. Inj Prev 1999;5:298-300. Crossref