Hong Kong Med J 2015 Apr;21(2):187.e3–4
DOI: 10.12809/hkmj144431
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Cor triatriatum: a rare cause of embolisation
KF Leung, FRCP (Edin, Glasg), FHKAM (Medicine); Alexson TK Lau, MRCP (UK), FHKCP
Department of Medicine, United Christian Hospital, Kwun Tong, Hong Kong
Corresponding author: Dr KF Leung (leungkwokfai@yahoo.com.hk)
 Full
paper in PDF
Full
paper in PDF
(1) The presence of cor triatriatum in the left atrium is shown by a portable echocardiogram machine at the apical four-chamber view.
(2) Flow accentuation across the fenestration in the cor triatriatum is shown by a standard echocardiogram machine at a modified apical four-chamber view.
(3) The presence of cor triatriatum is shown by transoesophageal echocardiogram at midoesophageal long-axis view.
Transthoracic echocardiogram was arranged for a
42-year-old woman who had been diagnosed with
ischaemic stroke in April 2013. While no thrombus
was found, a membranous structure with two
moderately sized fenestrations near the anterior and
lateral border of the left atrium was noted by portable
transthoracic echocardiogram (Fig a, Video [1]). Flow
accentuation with gradient up to 7 mm Hg across
the fenestrations and spontaneous echo contrast
were also documented by formal transthoracic
echocardiogram (Fig b, Video [2]) and transoesophageal
echocardiogram (Fig c, Video [3]). Computed
tomography of the heart with contrast was arranged
and the findings concurred with the echocardiogram
findings (Fig d). In addition to cardiac structural
abnormalities, the patient was noted to have atrial
fibrillation. The overall picture was compatible with
cor triatriatum, atrial fibrillation, and history of
embolic stroke. She refused both anticoagulation and
surgical excision of the cor triatriatum membrane at
the time of diagnosis. However, 2 months later, the
patient developed acute ischaemia of the right arm.
Computed tomography revealed a 4-cm filling defect
at the right proximal brachial artery. Echocardiogram
did not reveal any intra-cardiac thrombus. Surgical
embolectomy was successful in restoring the distal
pulses. Excision of the cor triatriatum along with
the modified Cox Maze III procedure and left atrial
appendage plication were subsequently performed.
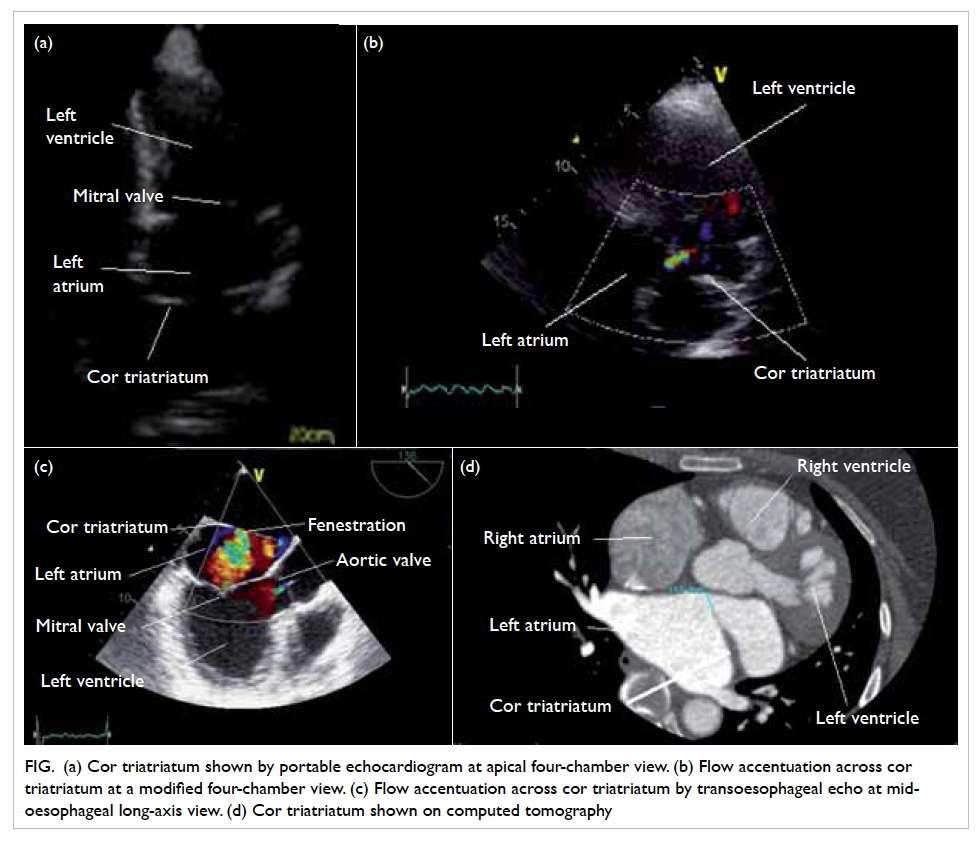
Figure. (a) Cor triatriatum shown by portable echocardiogram at apical four-chamber view. (b) Flow accentuation across cor triatriatum at a modified four-chamber view. (c) Flow accentuation across cor triatriatum by transoesophageal echo at mid-oesophageal long-axis view. (d) Cor triatriatum shown on computed tomography
Cor triatriatum is an uncommon congenital
anomaly. The left atrium is subdivided into a proximal
and a distal chamber by a fenestrated fibromuscular
membrane. The reported incidence is around 0.1% of
all congenital cardiac diseases.1 The most commonly
associated structural abnormalities in adults include
secundum atrial septal defect, mitral regurgitation,
and left superior vena cava with unroofed
coronary sinus.2 Patients present with symptoms
comparable to mitral stenosis due to their similar
haemodynamic effects with dyspnoea, orthopnoea,
and haemoptysis. Cardioembolic stroke is another
recognised complication and echocardiographic
features of embolic stroke, including left atrial
thrombus and spontaneous echo contrast, are
often found.3 Transthoracic echocardiogram is the
initial investigation of choice due to its accessibility.
Transoesophageal echocardiogram is needed
to define the structure precisely and to screen
for other co-existing congenital abnormalities.
Computed tomography of the heart can supplement
the echocardiographic findings before definitive
treatment.4 Open surgical resection of the accessory
membrane is indicated in patients with obstructive
symptoms. The procedure is performed through
median sternotomy and atriotomy according to
the morphology of the membranous defect and
co-existing abnormalities. The operative result is
excellent when patients present early and there are
no co-existing cardiac anomalies.5
References
1. Niwayama G. Cor triatriatum. Am Heart J 1960;59:291-317. Crossref
2. Reddy TD, Valderrama E, Bierman FZ. Images in
cardiology. Atrioventricular septal defect with cor
triatriatum. Heart 2002;87:215. Crossref
3. Park KJ, Park IK, Sir JJ, et al. Adult cor triatriatum
presenting as cardioembolic stroke. Intern Med
2009;48:1149-52. Crossref
4. Su CS, Tsai IC, Lin WW, Lee T, Ting CT, Liang KW.
Usefulness of multidetector-row computed tomography
in evaluating adult cor triatriatum. Tex Heart Inst J
2008;35:349-51.
5. Rodefeld MD, Brown JW, Heimansohn DA, et al. Cor
triatriatum: clinical presentation and surgical results in 12
patients. Ann Thorac Surg 1990;50:562-8. Crossref