Hong Kong Med J 2014 Dec;20(6):556.e4–5
DOI: 10.12809/hkmj134137
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Walker-Warburg syndrome: rare congenital muscular dystrophy associated with brain and eye abnormalities
CY Lee, FRCR, MB, ChB
Department of Radiology, Tuen Mun Hospital, Tuen Mun, Hong Kong
Corresponding author: Dr CY Lee (prodigycat@gmail.com)
 Full
paper in PDF
Full
paper in PDF
Case report
A 7-month-old boy was found to have developmental
delay, abnormal muscle tone, and abnormal eye
movement in December 2012. Physical examination
of the eyes revealed wandering gaze with convergent
squint. Ophthalmology was consulted and bilateral
retrolental masses were suspected. Blood tests
revealed elevated serum creatine kinase level.
Computed tomography of orbits showed
bilateral hyperdense retrolental tubular opacities
with small retinal haemorrhage on the right (Fig 1). Computed tomography of brain also showed
communicating hydrocephalus. Magnetic resonance
imaging of orbits showed deformed bilateral globes,
abnormal T1-weighted and T2-weighted hypo–to–iso-intense contrast-enhancing triangular bands with
base near the optic disc and apex at the posterior
surface of lens, compatible with bilateral persistent
hyperplastic primary vitreous. T1- and T2-weighted hyperintensity at right vitreous body
was compatible with previous haemorrhage.
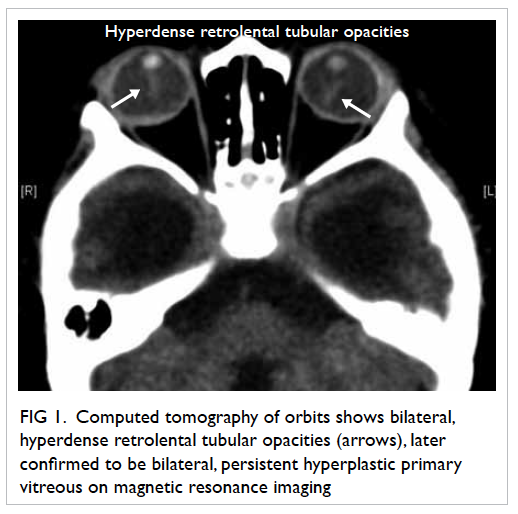
Figure 1. Computed tomography of orbits shows bilateral, hyperdense retrolental tubular opacities (arrows), later confirmed to be bilateral, persistent hyperplastic primary vitreous on magnetic resonance imaging
Magnetic resonance imaging of the brain
showed pachygyria, hydrocephalus, absent septum pellucidum, and hypoplasia of corpus callosum
forming type II lissencephaly (Fig 2). Mega cisterna magna, hypoplastic pons, and cerebellar vermis were compatible with posterior cranial fossa malformation
(Fig 3). Band-like structures in the bilateral periventricular regions with signal changes similar to grey matter were suggestive of band heterotopic grey
matter.
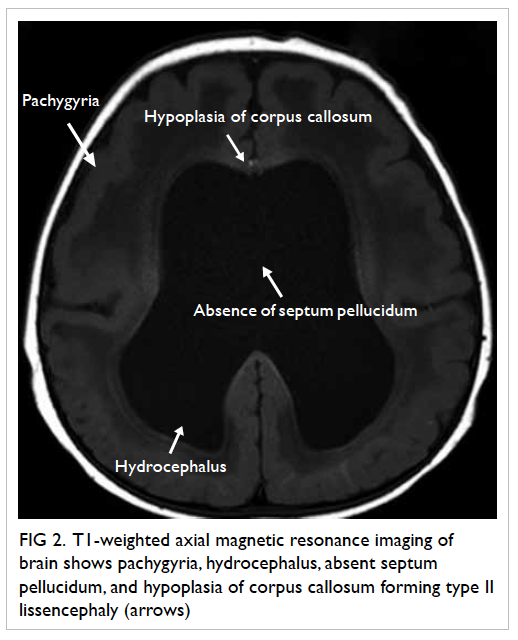
Figure 2. T1-weighted axial magnetic resonance imaging of brain shows pachygyria, hydrocephalus, absent septum pellucidum, and hypoplasia of corpus callosum forming type II lissencephaly (arrows)
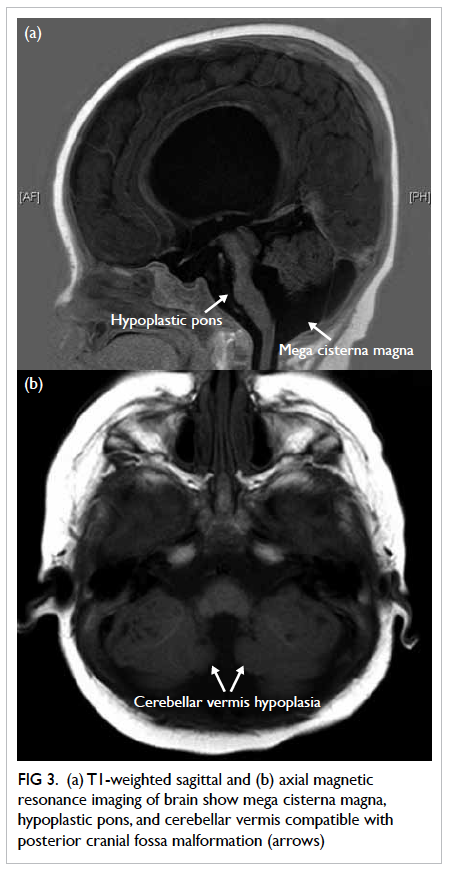
Figure 3. (a) T1-weighted sagittal and (b) axial magnetic resonance imaging of brain show mega cisterna magna, hypoplastic pons, and cerebellar vermis compatible with posterior cranial fossa malformation (arrows)
Radiological findings of type II lissencephaly,
posterior fossa malformation and retinal anomaly,
together with clinical findings of developmental
delay, abnormal muscle tone, and elevated serum
creatine kinase level were compatible with diagnosis
of Walker-Warburg syndrome.
Discussion
Congenital muscular dystrophy (CMD) comprises a
heterogeneous group of disorders. Walker-Warburg
syndrome is one phenotype of CMD known to occur
due to dystroglycanopathy,1 which is an autosomal
recessive condition. The overall incidence is unknown
but a survey in Northeastern Italy has reported an
incidence rate of 1.2 per 100 000 live births.2
Walker-Warburg syndrome affects the brain,
eye, and muscles with characteristic malformation.
Diagnostic criteria for Walker-Warburg
syndrome include type II lissencephaly, cerebellar
malformation, retinal malformation, and CMD.3 Common associated anomalies
include anterior chamber malformation of the eye
and hydrocephalus. The less commonly observed
anomalies include Dandy-Walker malformation,
cleft lip and palate, congenital macrocephaly or
microcephaly, posterior encephalocoele, ocular
colobomas, congenital cataracts, and genital
abnormalities. Neuroimaging findings other than
lissencephaly include band heterotopia, cerebellar
vermian hypoplasia, dysgenesis of corpus callosum,
abnormal white matter changes, hypoplastic cerebral
peduncles, intraventricular haemorrhage, cerebellar
polymicrogyria, collicular fusion, and fusion of
occipital poles.4 Laboratory investigations usually
show elevated serum creatine kinase level, myopathic/dystrophic muscle pathology, and altered alpha-dystroglycan.2
Differentiation of Walker-Warburg syndrome from other dystroglycanopathies, for example,
muscle-eye-brain disease or Fukuyama CMD, depends on the severity of
clinical presentation including motor function and intellectual disability, and involvement of the
central nervous system and eye.1 Walker-Warburg
syndrome is believed to be the most severe form of dystroglycanopathy with most children dying before
the age of 3 years.2 No specific treatment is available
for this syndrome. Management is mainly supportive and preventive.
References
1. Sparks S, Quijano-Roy S, Harper A, et al. Congenital
Muscular Dystrophy Overview. 2001 Jan 22 [Updated
2012 Aug 23]. In: Pagon RA, Adam MP, Ardinger HH,
et al, editors. GeneReviews® [Internet]. Seattle (WA):
University of Washington, Seattle; 1993-2014. Available
from: http://www.ncbi.nlm.nih.gov/books/NBK1291/.
Accessed Sep 2013.
2. Vajsar J, Schachter H. Walker-Warburg syndrome.
Orphanet J Rare Dis 2006;1:29. CrossRef
3. Dobyns WB, Pagon RA, Armstrong D, et al. Diagnostic
criteria for Walker-Warburg syndrome. Am J Med Genet
1989;32:195-210. CrossRef
4. Zaleski CG, Abdenour GE. Pediatric case of the day.
Walker-Warburg syndrome (cerebro-ocular dysplasia-muscular
dystrophy). Radiographics 1997;17:1319-23. CrossRef