DOI: 10.12809/hkmj144317
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
LETTER TO THE EDITOR
More compatible with ‘cryptic miliary tuberculosis’
CF Wong, FRCP (Edin), FHKAM (Medicine)
Tuberculosis & Chest Unit, Grantham Hospital, Aberdeen, Hong Kong
Corresponding author: Dr CF Wong (wongcf2001@yahoo.com.hk)
 Full
paper in PDF
Full
paper in PDF
To the Editor—I read with interest the case report
published by Shea and Ip titled “Pulmonary
tuberculosis complicating asbestosis”.1 On reading
the details, I could not agree on the authors’
interpretation of the findings and the diagnosis
of asbestosis. While it is beyond doubt that the
findings of calcified pleural plaques point towards
the diagnosis of a form of “asbestos-related pleural
disease”, this condition has to be distinguished from
‘asbestosis’ although the two conditions may co-exist
in some patients. Asbestosis refers to scarring
of the lung parenchyma as a result of heavy asbestos
exposure. Radiological features are usually in the
form of reticulation, linear and curvilinear opacities,
and parenchymal bands.2 These features were not
obvious in the computed tomographic images
shown. Rather, the prominent radiological findings
were those of fine nodules which, in my view, were
more compatible with a diagnosis of ‘cryptic miliary
tuberculosis’. Cryptic miliary tuberculosis is a form
of tuberculosis which tends to occur in the elderly
and presents with fever of unknown origin with
negative bacteriological findings.3 Diagnosis is
difficult and often delayed. Given the clinical and
radiological features of the case reported here, I think
a more appropriate title would be “Cryptic miliary
tuberculosis in an elderly patient with underlying
asbestos-related pleural plaques”.
References
1. Shea YF, Ip JJ. Pulmonary tuberculosis complicating
asbestosis. Hong Kong Med J 2014;20:265.e3-5. CrossRef
2. Roach HD, Davies GJ, Attanoos R, Crane M, Adams H,
Phillips S. Asbestos: when the dust settles an imaging
review of asbestos-related disease. Radiographics
2002;22:S167-84. CrossRef
3. Yu YL, Chow WH, Humphries MJ, Wong RW, Gabriel M.
Cryptic miliary tuberculosis. Q J Med 1986;59:421-8.
Authors’ reply
YF Shea, MRCP (UK), FHKAM (Medicine)1; Janice JK Ip, MB, BS, FRCR2
1 Department of Medicine, Queen Mary Hospital, The University of Hong Kong, Pokfulam, Hong Kong
2 Department of Radiology, Queen Mary Hospital, The University of Hong Kong, Pokfulam, Hong Kong
Corresponding author: Dr YF Shea (elphashea@gmail.com)
To the Editor—We would like to thank Dr CF Wong
for clarifying the terminologies used in our article.1
We apologise for not annotating the interstitial septal
thickening in the original figures; furthermore, the
resolution and greyscale of the images were not
optimal to demonstrate the reticulations in our case.
We have retrieved one of the baseline computed tomography (CT) images of the thorax of our patient
to further demonstrate the presence of interstitial
septal thickening on top of the calcified pleural
plaques (Fig). These findings signify that our patient
had lung parenchymal changes due to asbestos
exposure, together with asbestos-related pleural
plaques.2 Because of these parenchymal changes,
the diagnosis of tuberculosis was challenging in
the initial stage. We agree that ‘cryptic pulmonary
tuberculosis’ is more specific than ‘pulmonary
tuberculosis’ as the final diagnosis for our patient
who presented with pyrexia of unknown origin but
with apparently negative mycobacterial workup
at the beginning while the interval CT thorax
showed miliary shadows.3 Perhaps, ‘Cryptic miliary
tuberculosis in an elderly patient with asbestosis’
would be an even more accurate and attractive title
for this article. We would once again like to thank Dr
Wong for sharing his ideas and experience with us.
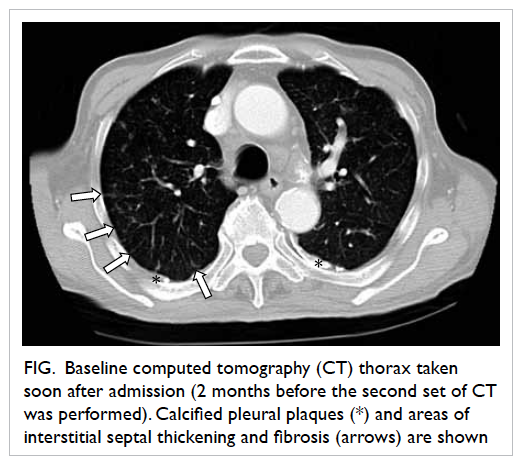
Figure. Baseline computed tomography (CT) thorax taken soon after admission (2 months before the second set of CT was performed). Calcified pleural plaques (*) and areas of interstitial septal thickening and fibrosis (arrows) are shown
References
1. Shea YF, Ip JJ. Pulmonary tuberculosis complicating
asbestosis. Hong Kong Med J 2014;20:265.e3-5. CrossRef
2. Fishwick D, Barber CM. Non-malignant asbestos-related
diseases: a clinical view. Clin Med 2014;14:68-71. CrossRef
3. Yu YL, Chow WH, Humphries MJ, Wong RW, Gabriel M.
Cryptic miliary tuberculosis. Q J Med 1986;59:421-8.