Hong Kong Med J 2014;20:264.e3–4 | Number 3, June 2014
DOI: 10.12809/hkmj/134018
© Hong Kong Academy of Medicine. CC BY-NC-ND 4.0
PICTORIAL MEDICINE
Fever with vesicular rash in an adult
Prashant Nasa, MD, FNB1; Ankur
Gupta, MD, DM2; Shakti Jain, MD3; Kishore
Mangal, MD, IDCCM1
1 Department of Critical
Care Medicine, Max Super Speciality Hospital, Shalimar Bagh, New
Delhi 110088, India
2 Department of
Nephrology, Max Super Speciality Hospital, Shalimar Bagh, New
Delhi 110088, India
3 Department of
Microbiology, Max Super Speciality Hospital, Shalimar Bagh, New
Delhi 110088, India
Corresponding author: Dr Prashant Nasa (dr.prashantnasa@hotmail.com)

A 30 year-old man was admitted with fever
and myalgia for 4 days, rashes over abdomen and forehead for 2
days (Fig 1), and breathing difficulty for 1 day
in January 2013. There was a history of similar rashes affecting
his wife 7 days earlier. On examination, he was tachypnoeic
(respiratory rate, 24 breaths/min), conscious, and oriented. He
had a papulo-vesicular rash on the forehead, scalp, and trunk but
the extremities were spared. Laboratory investigations revealed
thrombocytopenia (platelet counts, 30 x 109/L),
deranged liver function tests (serum bilirubin 4.6 mg/dL, direct
bilirubin 2.9 mg/dL, aspartate transaminase 1316 IU/L, alanine
transaminase 989 IU/L, alkaline phosphates 116 IU/L). The chest
X-ray showed no gross abnormality and the smear of skin scrapings
showed multinucleated epithelial giant cell (Tzanck cells),
abundant erythrocytes, and sporadic leukocytes (Fig
2). Aerobic bacterial culture of a swabbed vesicle fluid was
sterile. The history and characteristic pattern of the vesicular
rash on the scalp and abdomen with no history of childhood
immunisation against chickenpox clinched the diagnosis of
chickenpox. The diagnosis is primarily clinical. Confirmation
requires either viral culture of the vesicular fluid or direct
fluorescent antibody testing of serum,1
but these tests are not readily available. Smear examination
showing Tzanck cells in vesicle fluid may be positive in chicken
pox, but also occurs in herpes simplex, herpes zoster,
cytomegalovirus infection, and even pemphigus vulgaris.1 The differential diagnosis in our case was
severe Chicken pox, disseminated herpes simplex infection,
disseminated herpes zoster infection, drug eruptions, and
pityriasis lichenoides et varioliformis acuta. However the
clinical history (including family and vaccination history)
favoured severe chickenpox.
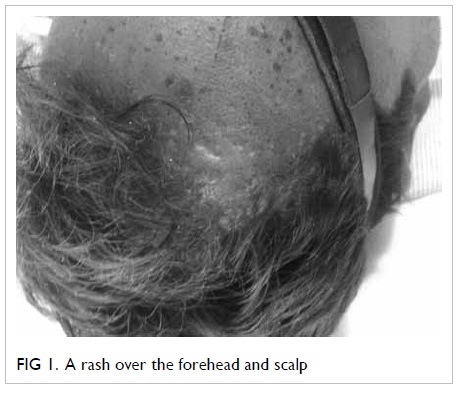
Figure 1. A rash over the forehead and scalp
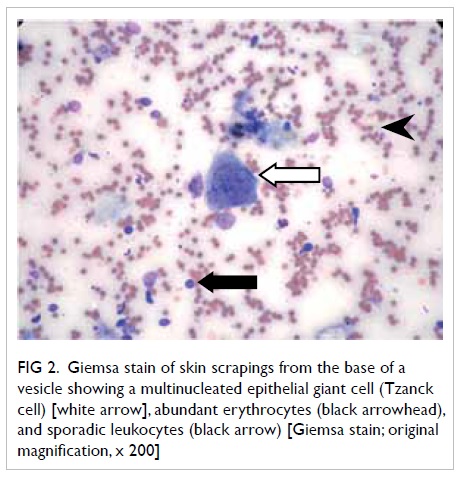
Figure 2. A Giemsa stain of skin scrapings from the base of a vesicle showing a multinucleated epithelial giant cell (Tzanck cell) [white arrow], abundant erythrocytes (black arrowhead), and sporadic leukocytes (black arrow) [Giemsa stain; original magnification, x 200]
Chickenpox is rarely fatal, although it is
generally more severe in adults than children; those who are
pregnant or immunocompromised have more severe forms of the
disease.2 Serious
manifestations of varicella-zoster virus (VZV) infection include
pneumonia, hepatitis, and encephalitis.2
3 The standard treatment
for severe adult VZV infection with or without involvement of
vital organs entails early recourse to intravenous antivirals such
as acyclovir. Whether severe or not, meticulous skin care,
hygiene, and droplet precautions should be implemented to prevent
cross-transmission to others till the patient’s lesions
desquamate.
References
1. Herpesviruses: Varicella zoster
virus (VZV). In: Shors T. Understanding viruses. 2nd ed.
Burlington, MA: Jones & Bartlett; 2011: 459.
2. Maggi U, Russo R, Conte G, et
al. Fulminant multiorgan failure due to varicella zoster virus and
HHV6 in an immunocompetent adult patient, and anhepatia.
Transplant Proc 2011;43:1184-6. CrossRef
3. Mohsen AH, McKendrick M.
Varicella pneumonia in adults. Eur Respir J 2003;21:886-91. CrossRef